
Vicki Shabo
Senior Fellow for Gender Equity, Paid Leave & Care Policy and Strategy, Better Life Lab
Federal FMLA and State Paid Leave Program Purposes, Utilization, Duration, and Family Care Coverage

This document has been updated multiple times since its original publication in June 2021 to reflect newly passed state paid leave programs, new data on state programs, and modified duration and family caregiving coverage. It will continue to be updated periodically as new information is available.
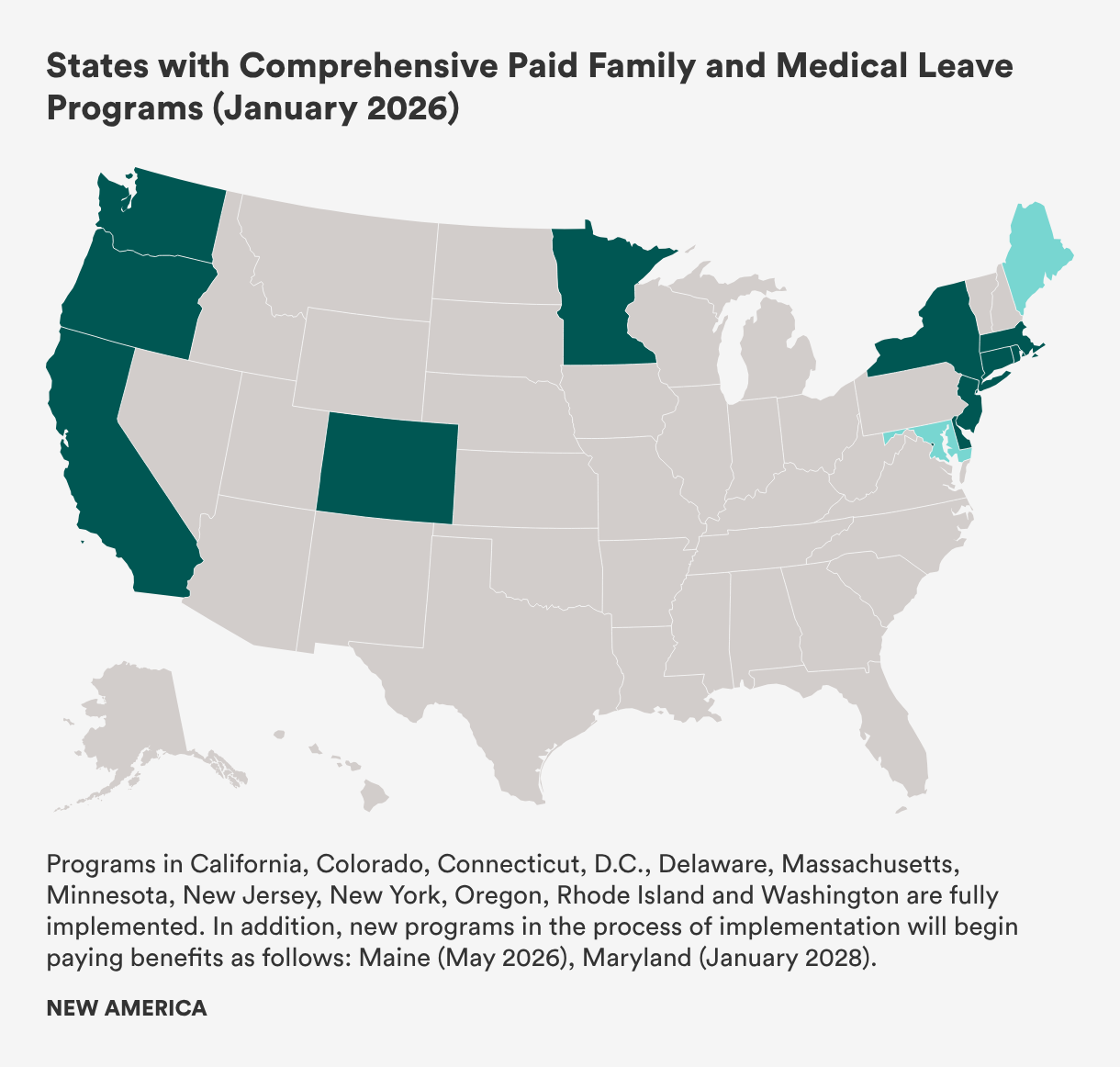
Comprehensive state paid leave programs currently or will soon support workers and employers in 13 states—California, Colorado, Connecticut, Delaware, Maine, Maryland, Massachusetts, Minnesota, New Jersey, New York, Oregon, Rhode Island, and Washington—and the District of Columbia when a qualifying need arises.[1] As of January 1, 2026, 12 of these programs are providing benefits now, and two others are in the process of being implemented.
More detail about benefit levels and funding streams for comprehensive state paid leave programs can be found in our companion piece, Paid Leave Benefits and Funding in the United States.
Research proves the value of paid family and medical leave. Yet at the federal level, and in U.S. states with the nation’s poorest measures of health and economic status, tens of millions of people are without paid leave when a serious personal or family health need arises or a new child joins a family. The nation’s first-ever permanent comprehensive paid family and medical leave program was included in the Build Back Better Act, which passed the U.S. House of Representatives in November 2021, but negotiations over this landmark legislation—which also included child care and home- and community-based care investments—stalled in the Senate.
In 2026, even as states reel from federal funding cuts to child care and early education, health care and food assistance, and more, state policymakers will continue to explore policy options for expanded access to paid leave. Strong bipartisan public and small business support for comprehensive policies—and best practices, lessons learned, and utilization data from various state policy approaches—should guide those efforts.
Ultimately, every working person and family in the United States needs access to paid family and medical leave, going beyond current federal law to guarantee income and job security to workers, as well as stability and certainty to businesses navigating an aging, caring workforce.
Since 1993, the Family and Medical Leave Act (FMLA) has guaranteed eligible workers up to 12 weeks away from their jobs to care for a seriously ill or injured parent, spouse, or child; to address their own serious health issue; or to care for a newborn, newly adopted, or newly placed foster child.[2] In the late 2000s, Congress amended the FMLA to cover two types of military caregiving leave: up to 26 weeks to care for a wounded service member by a parent, child, spouse, or next of kin, and up to 12 weeks for circumstances related to the deployment of a parent, spouse, or child. Despite proposals to expand access to the FMLA, Congress has not expanded the law since 2009.
The FMLA only provides unpaid leave to about 56 percent of the workforce due to exclusions based on business size and worker tenure; many workers’ inability to take leave without pay further limits eligible workers’ access. Workers who are paid low wages, single parents, rural workers, and Latine workers are less likely to be eligible for FMLA leave than other workers. But even with these barriers, the FMLA is estimated to have been used more than 460 million times in its first 30 years.
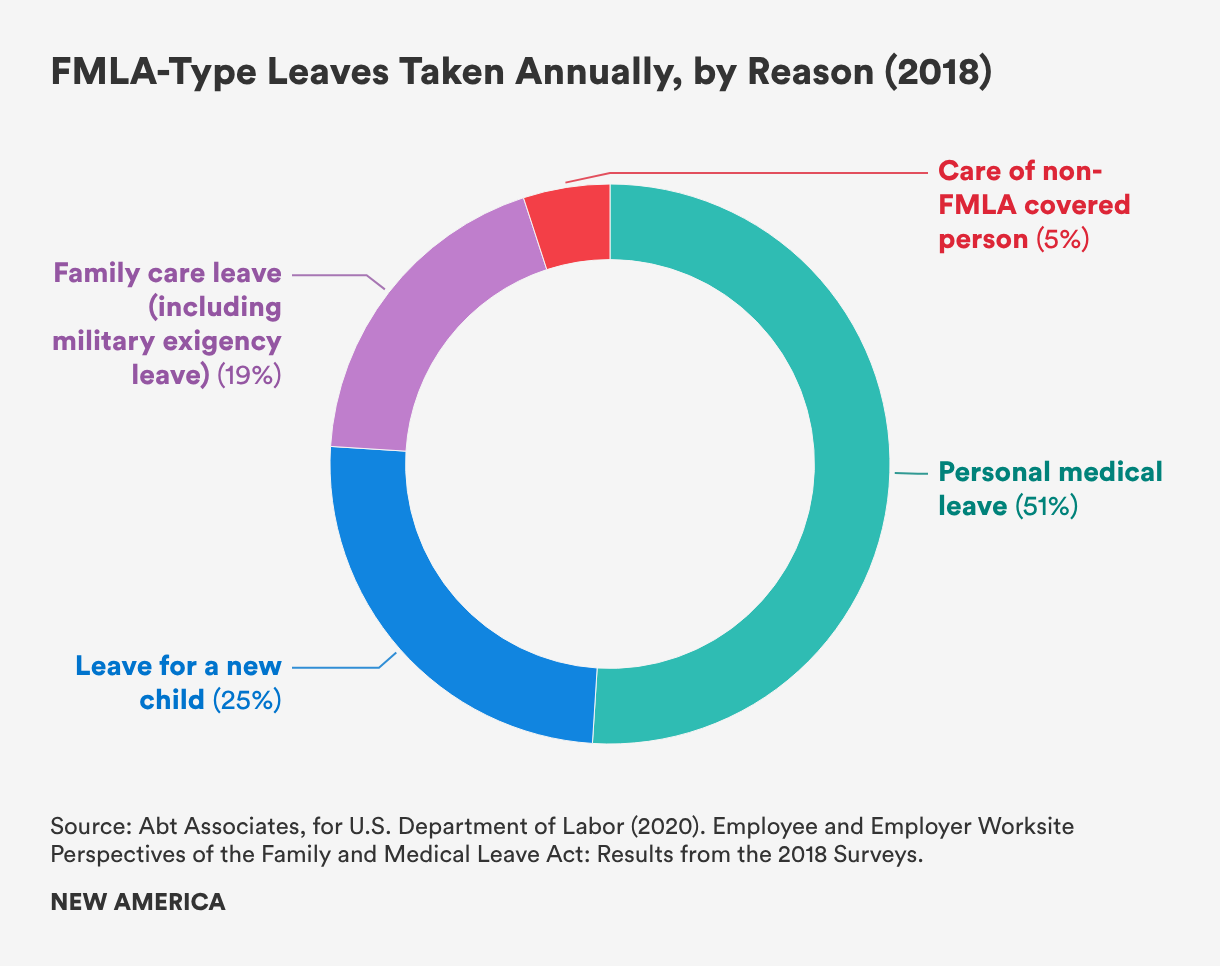
According to the U.S. Department of Labor’s most recent FMLA usage survey, 15.3 percent of the workforce takes leave for an FMLA-qualifying reason annually. Based on workers’ experiences in 2018, about half of all leaves workers take each year are for a serious personal medical issue (51 percent); one-fourth of all leaves are to care for a new child or address pregnancy-related needs (25 percent); one-fifth (19 percent) are to care for a seriously ill, injured, or disabled parent, spouse, or child or due to the deployment of a service member in the family; and 5 percent are to care for a family member not currently covered by the FMLA (for example, a grandparent, grandchild, sibling, or another extended family member).
The share of workers who need FMLA-type leaves far exceeds the share who are actually able to take leave to provide or receive care. In 2018, 6.9 percent of workers said they needed an FMLA-type leave but did not take it. This is a significant increase from 2012, when 4.6 percent of workers reported forgoing a needed leave. In each year, the most common reason people cited for not taking an FMLA-type leave they needed was their inability to afford unpaid leave (66 percent in 2018; 46 percent in 2012).
To build on the FMLA, 13 states plus the District of Columbia (DC) have or will soon have paid family and medical leave programs in place, which offer partial wage replacement to workers in businesses of all sizes. Each use of paid family and medical leave represents a parent who was able to care for a new child, a person who could get care for their own serious health issue without losing all of their pay, or a working family member able to care for a loved one.
Programs in DC and 11 states (California, Colorado, Connecticut, Delaware, Massachusetts, Minnesota, New Jersey, New York, Oregon, Rhode Island, and Washington) are fully implemented and paying benefits now, having collectively been used millions of times.
Maine’s program began collecting taxes in 2025 and will start paying benefits in May 2026. Maryland’s tax collection will begin in January 2027, and benefits will become available in January 2028.[3]
Legislation in California (passed in 2002, implemented in 2004), New Jersey (passed in 2008, implemented in 2009), Rhode Island (passed in 2013, implemented in 2014), and New York (passed in 2016, implemented in stages from 2018 through 2021) each added paid family leave benefits as a complement to long-standing temporary disability insurance that workers could use for wage replacement during a leave from work to address their own serious health condition, including pregnancy. Each of these programs has been updated one or more times since initial passage to better reflect workers’ needs. California recently implemented a major improvement to wage replacement rates, as well as the ability to file claims in advance, making the program much more accessible to lower- and middle-wage workers.
In 2017, Washington state and DC each passed new programs that were implemented in 2020. Despite launching during a global pandemic, each of these programs have successfully served workers and expanded their reach since initial passage.
In 2018, Massachusetts passed a program that went into effect in two stages in 2021: Massachusetts began making benefits available for personal medical needs, military leave, and caring for new children on January 1; and family caregiving benefits became available on July 1.
In 2019, Connecticut and Oregon adopted new programs. Connecticut’s program began collecting premiums in January 2021, accepting applications in December 2021, and paying benefits in January 2022. Oregon’s program began collecting premiums on January 1, 2023, and began paying benefits on September 3, 2023.
In 2020, Colorado became the first state to pass a paid leave program on the ballot by voter initiative. Premium collection began on January 1, 2023, and benefits became available on January 1, 2024.
In 2022, both Maryland and Delaware adopted new programs. Delaware’s program began collecting revenue in January 2025 and started paying benefits in January 2026. Maryland’s program implementation timeline has been pushed back due to unforeseen challenges largely unrelated to the program; contributions will now begin in January 2027, and benefits will start in January 2028.
In May 2023, Minnesota adopted a new program. Minnesota’s program began paying benefits on January 1, 2026. Minnesota is able to start benefits at the same time as the state begins collecting payroll contribution premiums, rather than collecting premiums first, by making general revenues available for benefits for a limited period of time.
In July 2023, Maine adopted a new program; the program was passed as part of a budget agreement. Maine’s program began collecting revenue in January 2025 and will start paying benefits in May 2026.
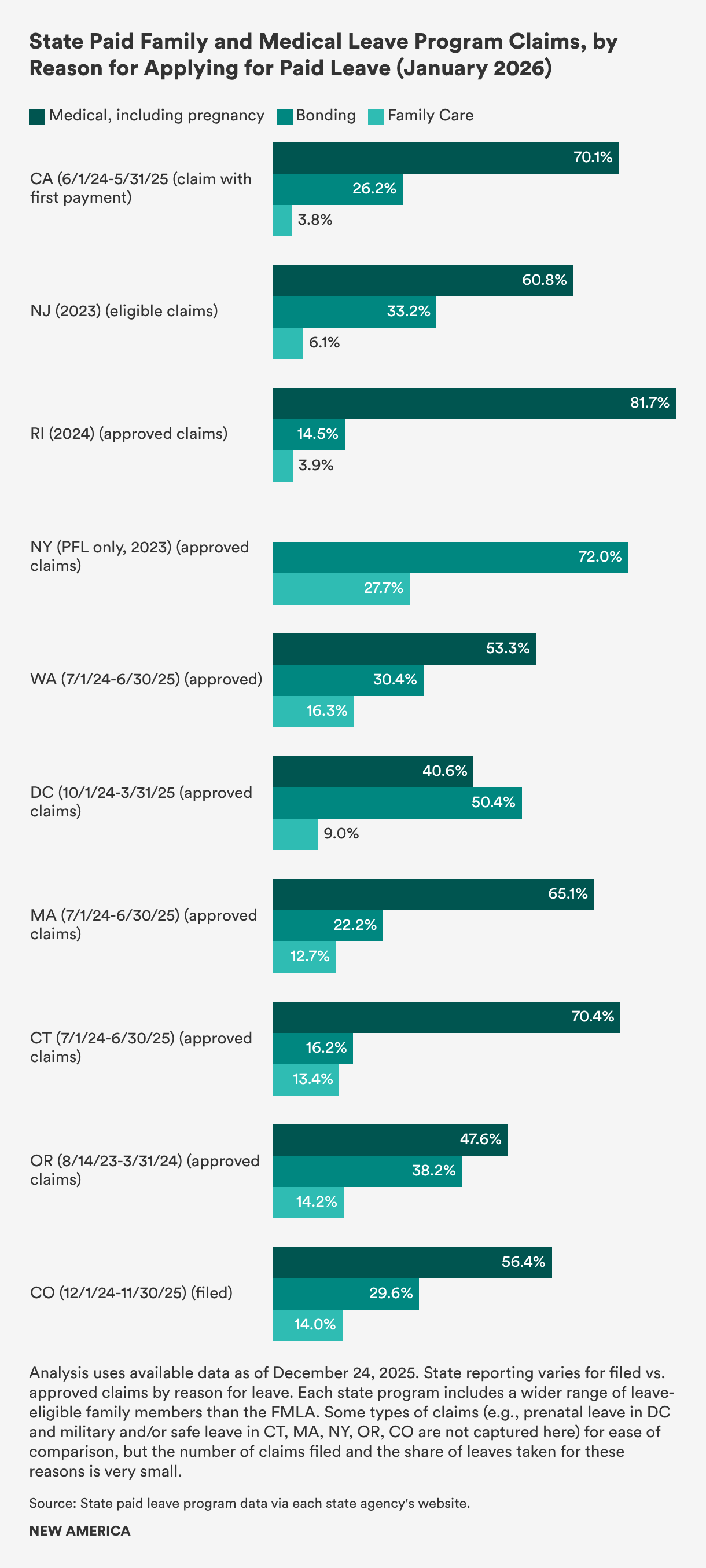
In most states, as with the federal unpaid leave program, personal medical leave is the most common reason workers use state paid leave programs, followed by caring for a new child through birth, adoption, or foster placement and caring for a family member.
In California, New Jersey, and Rhode Island, where temporary disability insurance programs that provide paid medical leave have been in place for decades, between 60 and 80 percent of all leave claims are filed for personal medical needs, including pregnancy and recovery from childbirth. In states that created programs from scratch, personal medical leave (including pregnancy-related leaves) tends to be between half and two-thirds of all claims, with the exception of DC, where medical leave utilization is lower, and Connecticut, where it is higher. Bonding with a new child accounts typically accounts for one-fifth to one-third of claims, but with significant variation between states with the lowest shares (Connecticut and Rhode Island) and the highest (DC).[4]
Family care leave is underutilized relative both to expected need and the unpaid FMLA, although several states saw small increases in the past year. Underuse may be because of waiting periods in some states, workers’ lack of awareness, the use of leave in short enough increments that the paperwork of applying for state paid leave may seem onerous, or other practical reasons.
The COVID-19 pandemic shows the utility of paid leave programs in a crisis. An Urban Institute analysis of California and Rhode Island state paid leave claim data from the first months of the COVID-19 pandemic concludes that these states’ programs were able to absorb a surge of new claims, making financial relief available to working families quickly and without unexpected costs on working people or their employers. Researchers from Stanford University, Columbia University, and the University of Virginia studying business impacts during the pandemic found increased support among small businesses for public paid leave programs.
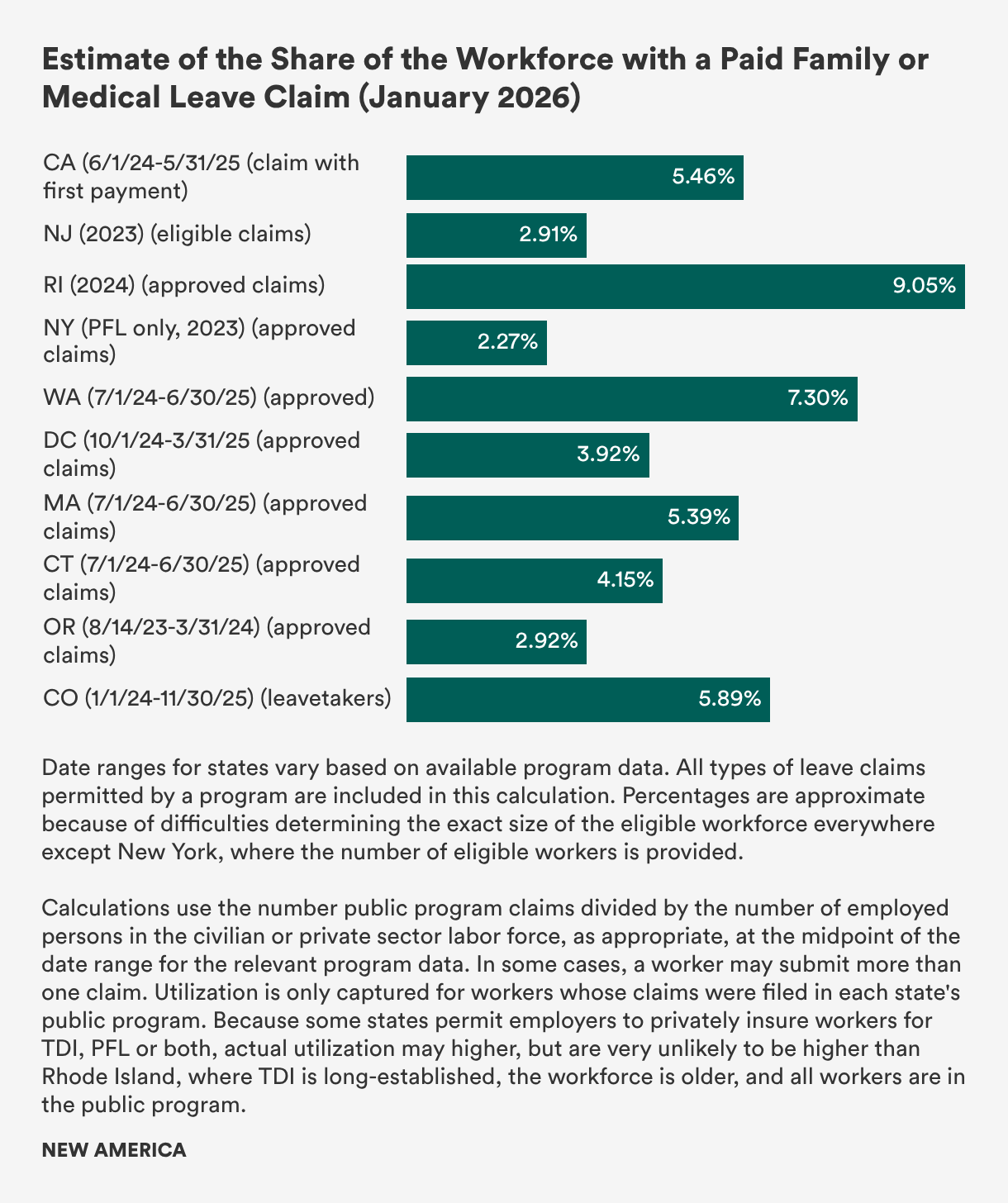
Program data show that a small share of workers (about 3 percent to 7 percent) use state paid leave programs each year, negating concerns sometimes raised about overuse or an untenable hit to a state’s workforce.[5] This is consistent with American Enterprise Institute–Brookings Institution utilization rate estimates in the three longest-standing paid leave states, California, New Jersey, and Rhode Island from 2016 to 2017.
Moreover, a growing body of research shows that paid family and medical leave is associated with greater workforce retention for new mothers; women providing care to loved ones, including caregiving for spouses; and workers with their own serious health issues such as cancer. Comprehensive paid leave is also estimated to reduce the share of workers who are poor, as well as to reduce utilization of other public benefit programs, according to Urban Institute research for the U.S. Department of Labor.
State paid family and medical leave programs offer workers time away from their jobs for a period of weeks or months. With the exception of new parents, especially women, who do tend make full use of the time available to bond with a new child, most workers do not take the full amount of time available to them—rather, they use the period of time they need to address their particular family or medical need and return to work expeditiously.
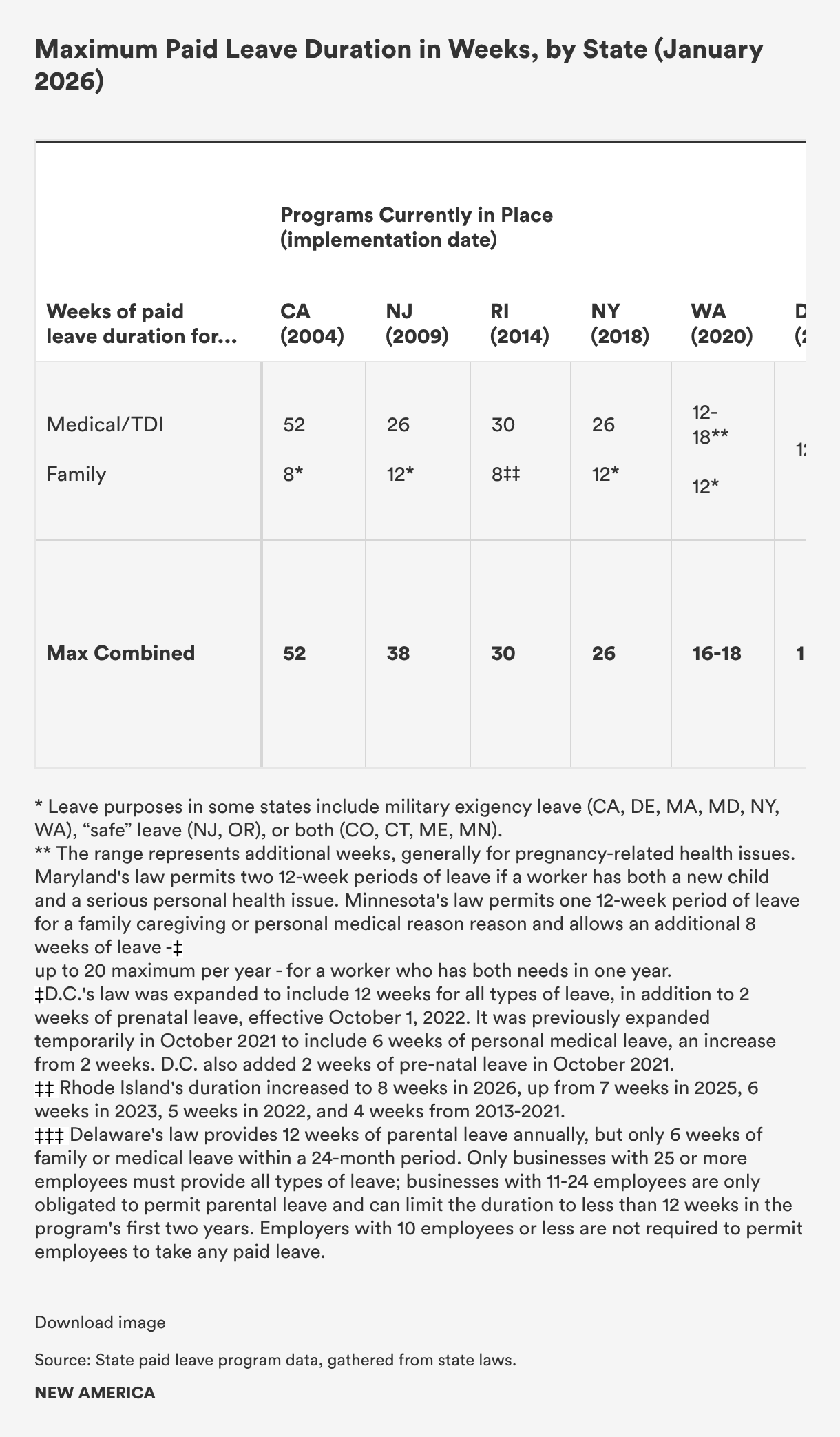
In California, New Jersey, New York, and Rhode Island, paid leave types are separated into two “buckets”: state temporary disability insurance (TDI) for personal medical leave and paid family leave (PFL) for new child and family care. These states’ TDI programs have been in effect for decades. They provide 26 weeks (New Jersey and New York), 30 weeks (Rhode Island), and 52 weeks (California) for people who need time away from their jobs to address a serious personal health issue, including pregnancy. Workers who use TDI typically use about one-third or less of the time available: between 10 and 16 weeks.
PFL programs in these four states complement TDI and offer PFL for between eight weeks in Rhode Island (which has increased leave from its original four weeks in one-week increments over time) and California (an increase from the state’s original provision of six weeks), and 12 weeks (New York, which scaled its duration over time as the program phased in, and New Jersey, which originally offered six weeks).
Washington was the first state to build a new program. Washington provides 12 weeks for parental leave or family care and 12 weeks for personal medical leave, with an additional two to four weeks available to people who have complications related to pregnancy, up to 16 or 18 combined weeks for all purposes in one year. Washington also allows parents grieving the loss of a pregnancy to take seven days of leave without a waiting period, as of January 1, 2023.
The District of Columbia also built and implemented a new program, which began providing benefits on July 1, 2020, but only for a limited number of weeks (eight weeks for new parents, six weeks for family caregivers, and two weeks for a worker to address their own serious health condition). The duration of leave available through DC’s program has been expanded twice since and, since October 1, 2022, DC provides up to 12 weeks for workers caring for a new child, a seriously ill or injured loved one, or their own serious health issue, with an additional two weeks for prenatal care.
Massachusetts’ program, effective in 2021, provides workers up to 26 weeks per year, which can be combined across multiple needs. Uses include up to 20 weeks for workers who need to address their own serious health issue; up to 12 weeks for leave to care for a family member or a newborn, newly adopted, or newly placed foster child; and up to 26 weeks for leaves related to care needs arising from a loved one’s military deployment. Beginning in late 2023, an amendment to the Massachusetts law means the commonwealth joins most other states in permitting employees to use their employer-provided paid leave benefits to “top off” their state-provided paid leave benefits.
Connecticut’s program began providing benefits on January 1, 2022. It offers workers’ benefits for up to 12 weeks (with two additional weeks available for people with pregnancy complications) to care for a new child, a loved one with a serious health issue, their own serious health issue, a family or personal domestic violence situation, or circumstances related to a loved one’s military deployment. In 2025, Connecticut expanded its program to include school paraprofessionals whose unique schedules previously rendered them ineligible.
Oregon’s program began paying benefits in September 2023. It offers workers’ benefits for up to 12 weeks (with two additional weeks available for pregnancy) to care for a new child, a loved one with a serious health issue, their own serious health issue, or a personal domestic violence situation. In 2024, Oregon made changes to its unpaid leave law to reduce the possibility of workers using paid and unpaid job-protected leave sequentially.
Colorado’s program began providing benefits on January 1, 2024. It offers workers’ benefits for up to 12 weeks (with two additional weeks available for people with pregnancy complications) to care for a new child, a loved one with a serious health issue, their own serious health issue, a family or personal domestic violence situation, or circumstances related to a loved one’s military deployment. In 2025, Colorado became the first state in the country to expand its program with an additional 12 weeks of leave for parents with babies in neonatal intensive care units.
Minnesota provides a base level of 12 weeks of paid leave, as will Maine, beginning in mid-2026, and Maryland, beginning in 2028. Maryland and Minnesota each allow workers who have both a personal health need and a family care need in a single year to access additional time, up to a maximum combined 24 and 20 weeks per year, respectively.
In Delaware, new parents can access up to 12 weeks of paid parental leave; people with family caregiving needs or personal health issues have six weeks available in a 24-month period.
Each state program except one recognizes a wide range of family members for whom workers may take leave to provide care and expands substantially on the FMLA’s parent, spouse, and child limitations on family caregiving. All but one include grandparents; all but one include siblings, with a 2026 expansion in Rhode Island that is now effective; and all but three include adult children and grandchildren. Parents-in-law are also included in all but three. Five of the newest laws and an expansion to New Jersey’s law include people who are related to the worker by blood or affinity, or “a significant personal bond” (commonly referred to as “chosen family”)—a provision of particular importance to LGBTQ+ people, Black and Latine families, and people with disabilities and their caregivers. Minnesota includes similar language, allowing family caregiving to be provided by “an individual selected by the incapacitated person.”

In sum, state paid family and medical leave programs expand substantially on FMLA by providing pay, additional coverage for caregivers, and, in some cases, longer leave durations. State programs, which are run in a sustainable, affordable way, provide strong models as federal lawmakers consider crafting a permanent national paid family and medical leave program.
[1] This explainer focuses on comprehensive paid leave programs but acknowledges the rise of voluntary models. At the federal level, a tax credit first enacted in 2017 and made permanent in 2025 reimburses employers a small amount for providing paid leave benefits to middle- and lower-wage workers available; in 2020, just 1,230 employers nationwide received this credit.
In addition, since 2022, two states provide insurance to state workers and allow employers and individual workers to opt in: New Hampshire’s program covers state employees and gives private employers the opportunity to purchase private insurance at insurer-set rates to cover six weeks of paid family and medical leave at 60 percent of a worker’s usual pay; workers whose employers do not choose to purchase insurance are able to buy a private insurance product on their own for no more than $5 per week. Employer enrollment in the program’s first two years has been extremely low, according to analysis by the University of New Hampshire Carsey School of Public Policy. Vermont launched a similar program in July 2023, enrolling state workers at that time and opening the program to private employers in July 2024. The Vermont program began allowing individual workers to self-enroll in July 2025.
In addition, eight states authorize the sale of private family and medical leave insurance. In 2022, Virginia authorized its State Corporation Commission’s Bureau of Insurance to approve the sale of family leave insurance products in the state; as of this writing in December 2025, only two insurers offer a family leave insurance product. Five states, Alabama, Arkansas, Florida, Tennessee, and Texas, passed similar laws based on an insurance industry model bill in 2023. Kentucky and South Carolina followed suit in 2024. These approaches are discussed in more detail at the end of our companion piece: Paid Leave Benefits and Funding in the United States and in the recent New America/National Partnership for Women & Families publication, Do Market Options Provide Time to Care? Evaluating Private Insurance-Based Approaches to State Paid Family Leave Access.
[2] Leave for one’s own serious health issue requires hospitalization or an incapacity lasting three or more days and continuing care by a health provider.
[3] Maryland’s program was initially set to begin collecting contributions in October 2023 and begin paying benefits in January 2025; the bill had passed in a veto override vote in 2022, and the outgoing administration did not make as much progress as was needed to meet this timeline. In 2023, 2024, and 2025, Governor Wes Moore signed legislation making some adjustments to the program and providing for a longer implementation timeline.
[4] Program claims data used for these calculations are for the most recent full year, or the most recently available year (New Jersey, Rhode Island, New York) or partial years (DC, Oregon), based on first-paid or approved claims except where noted for Colorado. New York does not report TDI take up for personal medical issues. Sources used are:
[5] Estimated share of the workforce using paid family and medical leave is based on the number of approved or first-paid claims from sources cited in Note 4 divided by the number of employed people in the civilian workforce for programs that cover some public sector workers, or the private sector, where programs only cover private sector workers. Employment data for some states (California, New Jersey, Rhode Island, Massachusetts, Connecticut, and Colorado) is likely to slightly overestimate the number of employed covered workers because of only partial or inconsistent coverage of public sector workers. In addition, the lack of wage or eligibility information for employed workers adds some additional uncertainty to these estimates in all states other than New York. Employment estimates were taken from the midpoint of the time period for paid leave claims, with sources and dates as follows:
Senior Fellow for Gender Equity, Paid Leave & Care Policy and Strategy, Better Life Lab



