
Table of Contents
Lack of Paid Leave as a Barrier to Care, Health, and Economic Security
A. The Importance of Paid Leave
Access to paid time away from work to provide care or seek health services for a loved one or one’s self is critically important for promoting good health, economic security, and well-being. Access to paid time away from work helps patients and caregivers access the treatments patients need.
For workers who are sick with contagious illnesses or need preventive health care services, access to paid sick time facilitates staying home, keeping sick children home, getting recommended immunizations and health screenings, and reduces rates of workplace injuries.1 Access to paid sick time also promotes efficient use of health care services and reduces emergency department use.2
For workers with serious health issues—and for workers who are family caregivers to loved ones with serious health issues—access to paid family and medical leave promotes compliance with treatment recommendations and reduces nursing home use.3 For example, nationally, an American Cancer Society-Cancer Action Network survey of employed cancer patients with access to paid leave found that workers who have and use paid leave are significantly more likely than others to complete treatment, go to medical and treatment appointments, manage symptoms and side effects, exercise choice over where to get treatments and which treatments to get, and afford treatment.4 A small qualitative study of women cancer survivors in rural Illinois found that access to paid sick time and paid medical leave was one contributor to remaining employed during and after treatment; in contrast, employed cancer patients who used FMLA unpaid leave—who tended to be in lower-quality jobs with less secure employment—were more likely to use the leave and then exit work.5 For caregivers of cancer patients, having and using paid leave is associated with a higher likelihood of going to a loved one’s appointments and treatments, helping with a loved one’s care, and addressing their own health issue.6
For new parents, access to paid family leave results in more time spent with children, which contributes to better child and maternal health, greater engagement by fathers in their children’s lives, and higher rates of women’s employment, and higher earnings.7 Paid leave also plays an important role in promoting health for babies in the NICU and children who are hospitalized.8 One meta-analysis of NICU children found that more maternal care in a NICU contributes to maternal-child bonding, better infant health outcomes, better maternal mental health and more success with breastfeeding.9
B. Prior Research on Access to Paid Leave Nationally and in Rural America
The United States is one of the only countries in the world that does not guarantee any form of paid sick time or paid family and medical leave to workers. The Family and Medical Leave Act of 1993 (FMLA) provides job-protected, unpaid leave for up to 12 weeks per year, but only to certain workers with serious health conditions or who are caring for a new child or a parent, spouse, or child with a serious health condition.
Nationally, the FMLA only covers an estimated 56 percent of the workforce, because its requirements that employees be provided job-protected leave and continued health insurance benefits only apply to worksites with 50 or more employees within a 75-mile radius. Furthermore, even within covered worksites, employees must have worked for at least one year for the employer and logged 1,250 hours in the past year to be eligible for FMLA protections.10
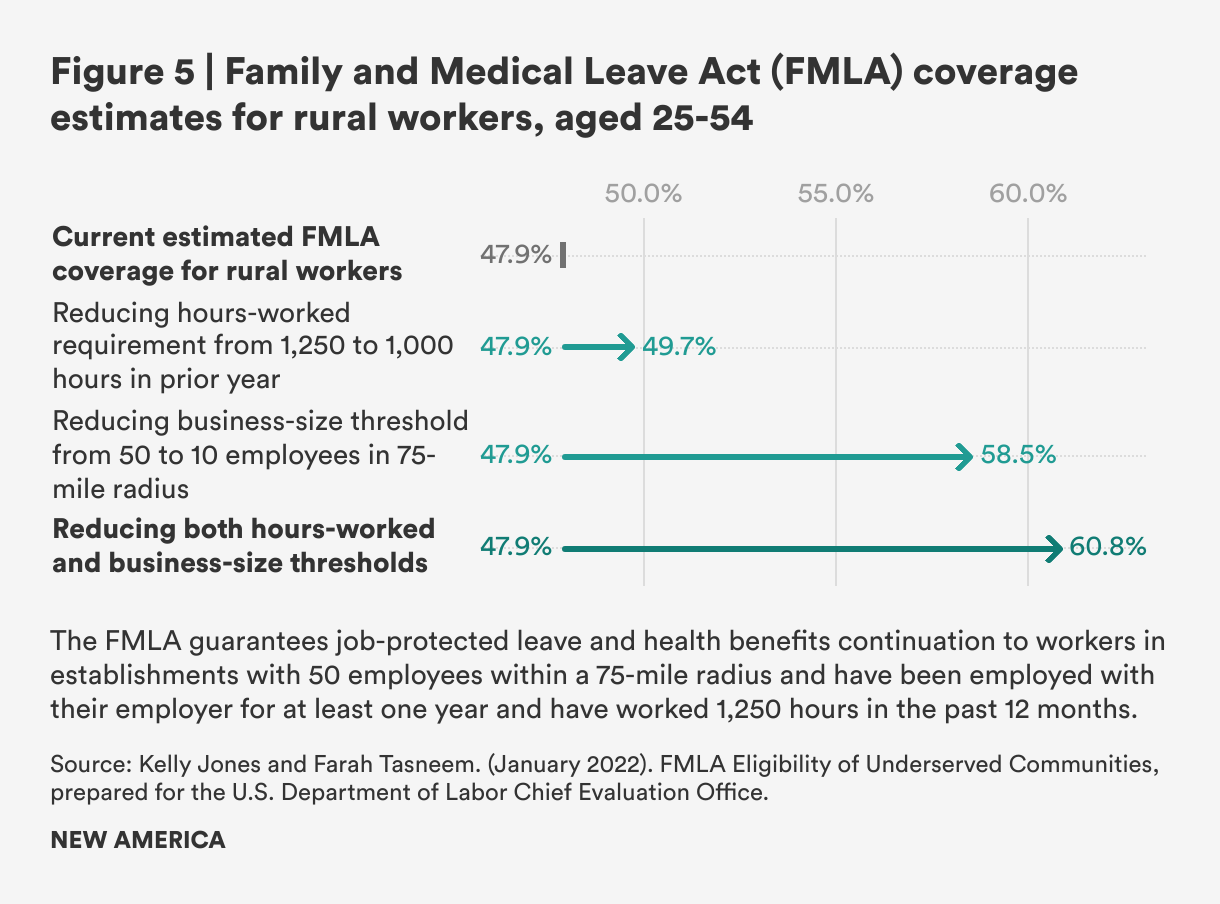
Rural workers’ FMLA coverage rates are estimated to be lower, primarily due to the firm size requirements: A simulation of FMLA access for workers aged 25-54 in rural communities estimates FMLA access for just 47.9 percent of rural workers compared to 51.4 percent for workers aged 25-54 overall under current law, and predicts expanded access with a reduction in the hours-worked requirements to 1,000 hours (49.7 percent coverage and eligibility for rural workers), a drop in the business size threshold to 10 employees (58.5 percent coverage and eligibility for rural workers), or both (60.8 percent coverage and eligibility for rural workers).11
Some U.S. states have done better than the federal floor. Twenty states and the District of Columbia have adopted more generous job protection requirements that apply to employees in smaller workplaces and workers with fewer hours or less job tenure.12 Eleven states and the District of Columbia have created paid family and medical leave social insurance programs, to guarantee paid leave to working parents and family caregivers and to workers with their own serious health issues through worker and/or employer-funded social insurance programs.13 And more than a dozen states, the District of Columbia, and two dozen localities have adopted their own paid sick days laws, which require employers to provide earned paid sick time to employees based on the number of hours an employee works.14
Notwithstanding state progress, without federal requirements or systems in place, most workers’ access to paid leave is left to the discretion of their employers. Overall in the United States, as of March 2022, 25 percent of civilian workers and 24 percent of private-sector workers had paid family leave through their jobs to care for a new child or a seriously ill loved one; 41 percent (civilian) and 43 percent (private sector) had temporary disability insurance, which is a form of personal medical leave, for extended personal serious health needs, including pregnancy and recovery from childbirth; 79 percent (civilian) and 77 percent (private) had paid sick leave. Access to benefits varies dramatically by wage level, industry and employer size—with lower-wage workers, service- and front-line occupations and workers in smaller companies less likely to have access.15
“Just 24 percent of private-sector workers nationwide had dedicated paid family leave through their jobs in 2022.”
Demographics, industry, business size, and unionization have been found to significantly affect workers' access to paid time away from work for health and caregiving needs in rural communities, but geography itself also plays a role in workers’ access to paid leave and other family-supporting benefits. For example:
- A 2009 study, using data from 2000-2006, found sizeable gaps in rural mothers’ access to paid sick and vacation days—as well as lower median earnings, lower levels of education, and lower unionization rates, but similar average labor market experience, hours worked, and share employed by the public sector. The study analyzed disparities in working mothers’ access to leave and found that about half of the difference was due to work establishment size, occupation, industry, and unionization. Even controlling for these factors, however, there were still significant differences in access among workers in sales occupations and among mothers in both very small (under 25 employees) and very large (500 or more employees) work establishments, with rural mothers’ access significantly less common than urban mothers’ access.16
- Researchers analyzed 2008 data from the National Study of the Changing Workforce and found that rural workers were significantly less likely to report having access to at least five paid sick days, and that rural parents were less likely to report having at least five paid sick days to care for a sick child. The gaps were especially pronounced in the private- and non-profit sectors. Disparities were reduced but not eliminated when controlling for full-time work hours and persisted when controlling for workplace and demographic characteristics, leading researchers to conclude that geography itself was a significant factor in the different rates of access.17
- A 2014 study of cancer patients in Vermont found that a smaller share of rural patients reported using paid disability leave relative to urban patients (12.3 percent versus 17.9 percent). Even after controlling for age, education, and cancer stage, rural workers were 33 percent less likely to use paid disability leave. The study authors noted that the types of manual labor jobs in rural communities are less likely to offer paid medical leave and that this may increase the negative impact of cancer diagnoses on rural workers and contribute to their 66 percent greater likelihood to retire early after a diagnosis, controlling for age, education, and cancer stage.18
- A 2015 analysis of a multi-decade longitudinal pooled sample of women surveyed as part of the National Longitudinal Study of Youth, from 1989 through 2020, provided insights on access to a range of family-supportive benefits. Researchers found that rural women’s odds of reporting access to paid maternity leave was 24 percent lower than urban women; the odds of rural women reporting access to paid vacation time was 20 percent lower, paid sick leave 13 percent lower, and flexible work scheduling 11 percent lower than urban women. For each benefit other than paid sick leave, workplace factors did not explain the disparities, while for paid sick leave, the size of employer and unionization explained the differences.19
Additionally, a recent analysis of the 2020 National Health Interview Study, which we also use in one of our analyses below, examined full-time rural workers’ access to paid sick time and found that rural workers’ access to paid sick days was 10 percentage points lower than urban workers’ access (68.1 percent versus 77.1 percent). Significant and large differences persisted even after adjusting for socio-demographic characteristics including age, gender, marital status, race and ethnicity, education, health status, and hours worked.20.
The 2020 NHIS data analysts concluded, “The geographic inequities we identified in access to paid leave compound other structural barriers to good health that rural residents experience.”21 They found that the workers least likely to have access to paid sick leave are 18-24 year olds, never-married people, Hispanic people, adults with a history of diabetes or stroke, and people who rate themselves as in fair or poor health. Rural workers with less than a high school degree, who make up a small but disproportionate share of the rural workforce, have particularly low rates of access, and experience significant gaps relative to their urban counterparts; lower predicted probabilities persist even at higher levels of educational attainment controlling for other factors.22
C. Additional Insights on Access to Paid Leave in Rural America
Our original analyses below add to the evidence that rural workers, and particularly rural Hispanic/Latine workers, have less access to paid sick time and paid family and medical leave than non-rural workers. We examined data from the 2019 National Health Interview Survey (NHIS) to examine access to paid sick time and the 2017-2018 American Time Use Survey (ATUS) to examine access to paid leave for family and medical reasons consistent with the FMLA.23 In addition to analyzing access between rural or "non-metropolitan" areas and metropolitan areas overall and by gender and race, we also examined access among residents of areas with a high share of people in poverty and within 200 percent of the federal poverty line. We use the terms Hispanic and Latine interchangeably in our analysis, though we note that the surveys use the terminology "Hispanic."
We note that both the NHIS and the ATUS have limitations in terms of the questions that are asked. We are unable to assess the quality or duration of the paid sick leave provided through the question asked on the NHIS. The ATUS asks about any paid time off that can be used for particular purposes, not whether that time is specifically designated for a unique purpose or the duration of the available paid leave. In addition, we note that the definition of “rural” each study uses is different because of the different rural definitions used by the Census Bureau and the U.S. Department of Health and Human Services, so these results cannot be compared to one another. In the final section of this report, we recommend better surveys for data collection on these topics.
1. Paid Sick Time
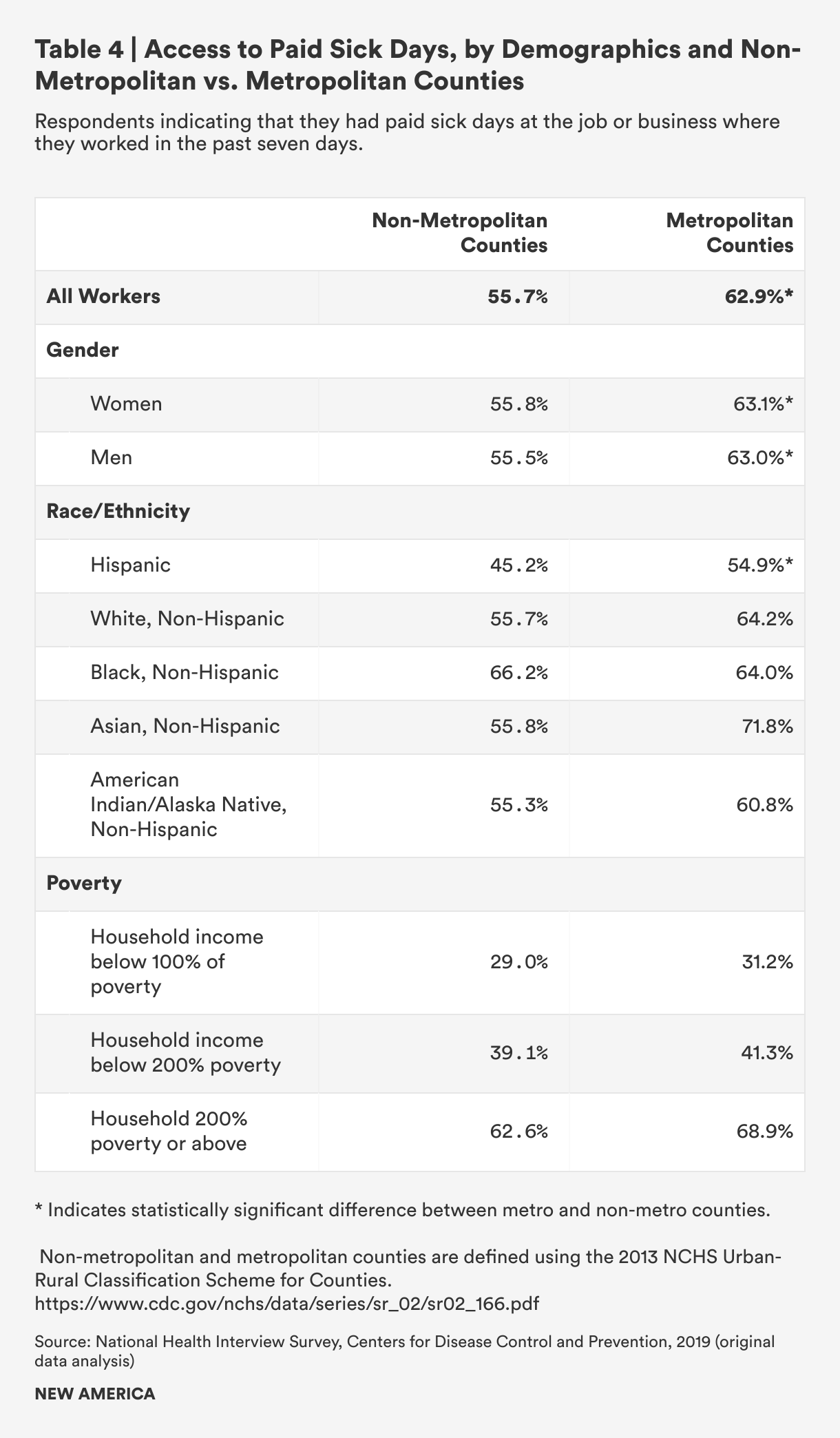
The NHIS asks respondents whether they have paid sick leave at the job or business they worked in during the past seven days. The NHIS data for all workers in rural counties (“non-metropolitan counties”), similar to the Henning-Smith NHIS analysis of full-time workers discussed above, shows a statistically significant 7-percentage point difference in access to paid sick time among rural and non-rural workers. Just over half of rural workers (55.7 percent) compared to more than six-in-ten workers in metropolitan areas (62.3 percent) reported access to paid sick time at the job they spent the most time at in the previous week.

Women and men were about equally likely to report access to paid sick time in both rural and metropolitan areas and to experience the same 7-point rural-metropolitan gap. Access is lowest among rural Hispanic workers (just 45 percent report access to paid sick leave), and the rural-metropolitan gaps are largest among Hispanic workers (9.6 percentage points) and non-Hispanic white workers (8.5 percentage points). Black workers’ access to paid sick time is about the same in rural and non-rural areas. There are big gaps among Asian people in rural versus non rural areas, but the small sample size means that the 16-percentage point gap is not statistically significant; differences in rural versus non-rural access are smaller for American Indian and Alaska Natives (AIAN) (6 percentage points) and not statistically significant. When Asian people, AIAN people and “others” are combined, the gap between rural and non-rural access is large, with rural people 11 percentage points less likely to have access to paid sick time, and it is a statistically significant difference.
The gap between rural and urban workers persists, but does not grow, among people whose household income is at the federal poverty line or at 200 percent of the federal poverty line. Access to paid sick leave among lower-income rural and metropolitan workers is low: fewer than one-third report access to paid sick time at their jobs. But for rural workers, who must travel further for health care services, lack of access to paid time off may involve particular economic burdens and employment risks.
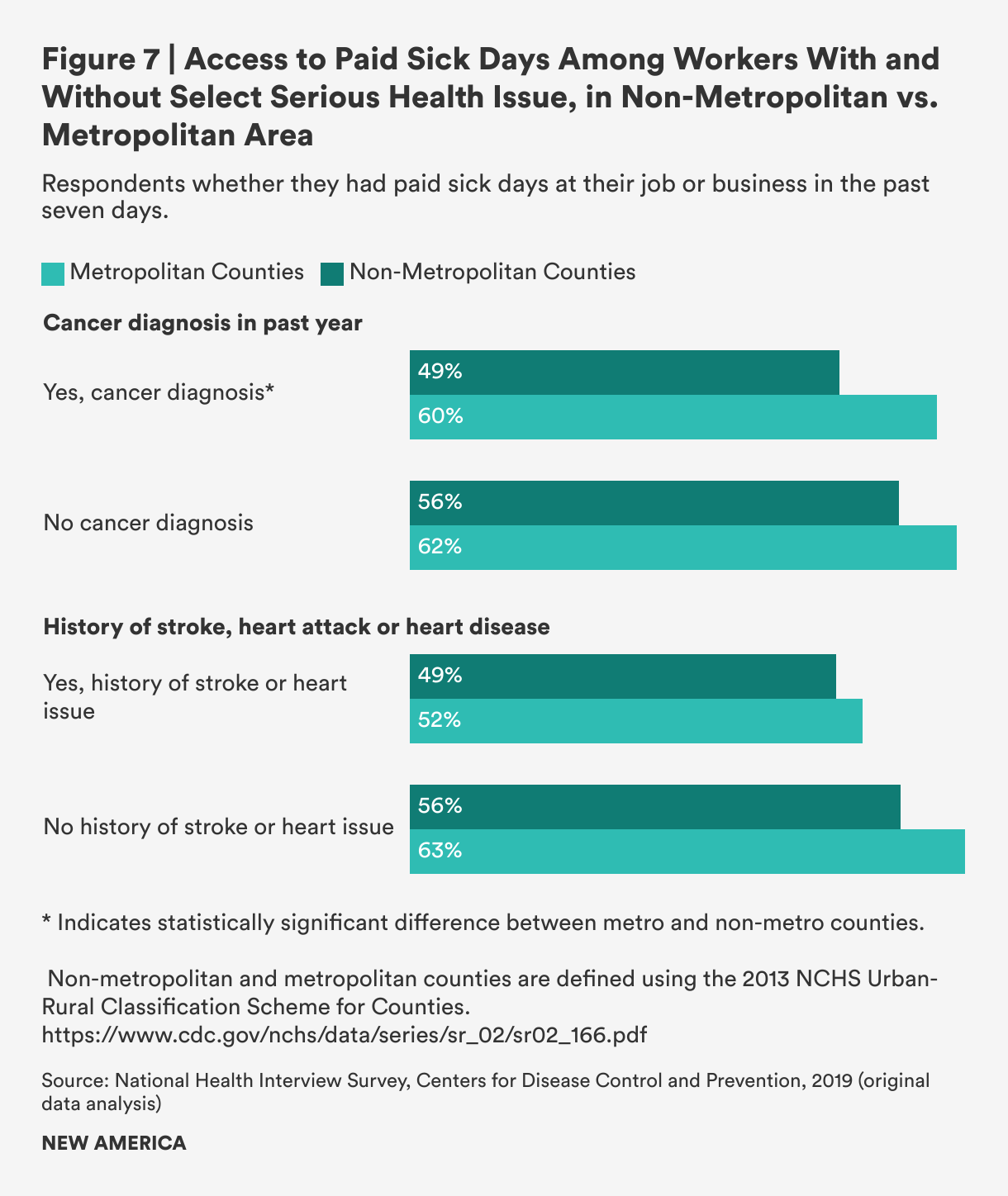
We also examined whether workers with serious health issues in rural and metropolitan areas had differential access to paid sick time. Importantly, we found that workers who reported having a cancer diagnosis in the past year were less likely than those who did not to have paid sick leave, and for rural workers, access was even lower. Just under half of rural workers who reported a cancer diagnosis in the past year said they had access to paid sick leave at their job (49 percent), compared to rural workers who were cancer-free (56 percent) and compared to both metropolitan area workers with a recent cancer diagnosis (60 percent) and metropolitan workers without a recent cancer diagnosis (63 percent). We did not find any similar geographic associations with workers who have cardiovascular diseases like strokes or heart disease—though smaller shares of both urban and rural workers with cardiovascular disease report access to paid sick leave; this is likely the result of socioeconomic status, industry, and occupation.
2. Paid Leave for Family or Medical Needs
Workers’ inability to access paid leave during a period of serious illness or care needs has implications for most families and households. In 2018, a national public opinion survey asked voters across the country how likely they would be to face a “serious financial hardship” if they had to take up to a few months of unpaid time off from their job because of a serious illness or injury, to care for a new child, or to care for a family member with a serious illness, injury, or disability. More than half of rural residents said they would be “very likely” to face a serious financial hardship—12 percentage points more than people in metropolitan areas.24
The ATUS provides the only federally-collected data at a large enough scale to analyze access to paid leave by rural and non-rural communities. The questions asked are imperfect for the purposes of quantifying access to designated paid family and medical leave; respondents are asked whether they have access to “any paid leave” and then a series of questions about the purposes for which they can use the leave, including the birth or adoption of a child, eldercare, the illness or medical care of a family member, or their own illness or medical care, but respondents may be thinking about paid vacation, personal or sick time that can be used for these purposes and which may be of a limited duration.
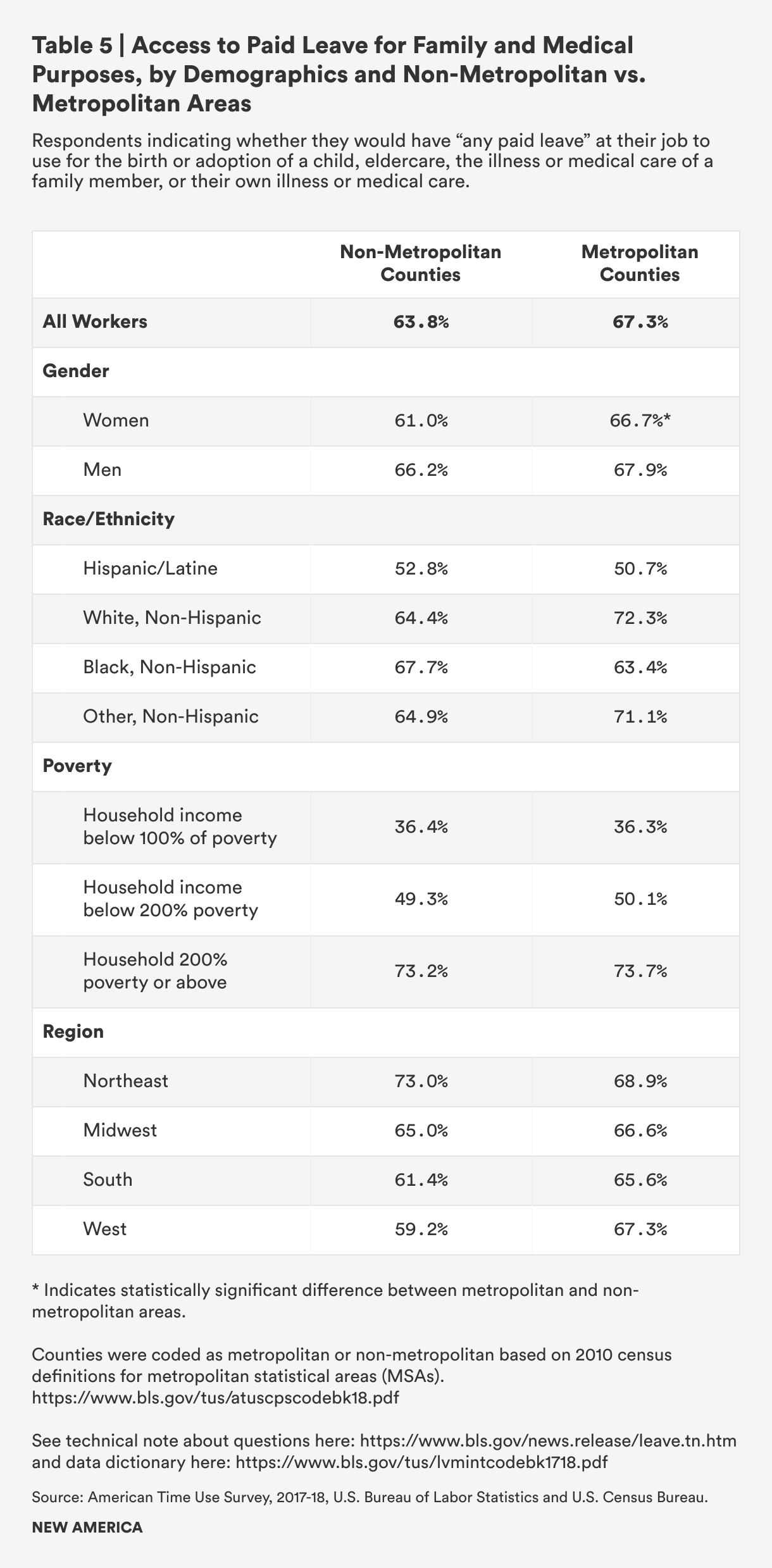
We find that 64 percent of workers in rural areas said they would have paid leave to use for these family and medical leave-type purposes if they needed it, compared to 67 percent of metropolitan area workers. Rural men and metropolitan men have about equal access, whereas just 61 percent of rural women report paid leave access compared to 67 percent of metropolitan women.

Hispanic people in both rural and non-rural areas report low levels of access—just 53 percent of rural Latine people and 51 percent of metropolitan Latine people report access to paid leave to use for family and medical needs. However, there are statistically significant and substantial gaps among rural white people compared to metropolitan-area white people (64 percent access in rural areas compared to 72 percent in metro areas). There are also gaps for people of other races, including Native, Asian, Pacific Islanders, and multiracial people (65 percent access in rural areas compared to 71 percent in metro areas), but these are not statistically significant. Black people are an outlier, and this may be related to public-sector versus private sector employment: rural Black workers have higher access rates compared to metro-area Black workers (68 percent versus 64 percent), but this difference is also not statistically significant.
People who live at the poverty level are equally unlikely to have paid leave for family and medical reasons, whether in rural or metropolitan areas (36 percent) or at 200 percent of the poverty level (49 percent in rural counties and 50 percent in metropolitan counties), but the barriers to providing care may be greater in rural areas because of travel distances and a shortage of care providers.
Workers in rural areas of the west (59 percent), south (61 percent) and Midwest (65 percent) have less access to paid leave than Northeastern rural workers (73 percent). There is also a sizable differential between rural and non-rural workers in the west (59 percent versus 67 percent) and a smaller but still meaningful difference among rural and non-rural southern workers (61 percent versus 66 percent).
Citations
- National Partnership for Women & Families, Paid Sick Days Improve Public Health (Washington, DC, 2021), source.
- Yanlei Ma, Kenton J. Johnson, Hao Yu, Frank J. Warham, and Hefei Wen, "State Mandatory Paid Sick Leave Associated With A Decline In Emergency Department Use In the US, 2011-2019," Health Affairs 41 (8) (2022), source.
- Diana Boesch, Quick Facts on Paid Family and Medical Leave (Washington, DC: Center for American Progress, 2021), source.
- Public Opinion Strategies, Interested Parties Memorandum: Key Findings – National Surveys of Cancer Patients, Survivors and Caregivers (2017), source.
- Hallgren et al., “Facilitators and barriers to employment for rural women cancer survivors.”.
- Public Opinion Strategies, Interested Parties Memorandum.
- Jane Waldfogel, Elizabeth Doran, and Jessica Pac, Paid Family and Medical Leave Improves the Well-Being of Children and Families (Washington, DC: Society for Research in Child Development, 2019), source.
- Ashley Weber, Tondi M. Harrison, Deborah Steward, and Susan Ludington-Hoe, "Paid Family Leave to Enhance the Health Outcomes of Preterm Infants," Policy, Politics, & Nursing Practice (August 22, 2018), source; Jody Heymann and Allison Earle, Raising the Global Floor: Dismantling the Myth That We Can't Afford Good Working Conditions for Everyone (Stanford, CA: Stanford Politics and Policy, 2010).
- Susanne Klawetter, Jennifer C. Greenfield, Stephanie Rachel Speer, Kyria Brown, and Sunah S. Hwang, "An integrative review: maternal engagement in the neonatal intensive care unit and health outcomes for U.S.-born preterm infants and their parents," AIMS Public Health 6 (2) (2019): 160–183.
- Brown et al., note 29, 7.
- Kelly Jones and Farah Tasneem, “FMLA Eligibility of Underserved Communities,” Working Paper Produced for the U.S. Department of Labor Chief Evaluation Office (January 2022), 15 (Table 3), source.
- National Partnership for Women & Families, Raising Expectations: A State-by-State Analysis of Laws That Help Working Family Caregivers, (Washington, DC, 2018), source.
- Vicki Shabo, Explainer: Paid Leave Benefits and Funding in the United States (Washington, DC: New America, 2022), source; A Better Balance, Comparative Chart of Paid Family and Medical Leave Laws.
- National Partnership for Women & Families, Current Paid Sick Days Laws.
- U.S. Bureau of Labor Statistics, National Compensation Survey.
- Rebecca Glauber, Family-friendly Policies for Rural Working Mothers (Durham, NH: Carsey Institute, University of New Hampshire Policy Brief No. 15, Summer 2009), source.
- Kristin Smith and Andrew Schaefer, Rural Workers Have Less Access to Paid Sick Days (Durham, NH: Carsey Institute, University of New Hampshire Policy Brief No. 32, Summer 2011), source
- Snowden, Vacek, and Geller, “The impact of cancer diagnosis on employment.”
- Rebecca Glauber and Justin Robert Young, "On the Fringe: Family-Friendly Benefits and the Rural—Urban Gap Among Working Women," Journal of Family Economic Issues 36 (2015): 97-113.
- Carrie Henning-Smith, Janette Dill, Arianne Baldomero, and Katy Bakes Kozhimannil, "Rural/urban differences in access to paid sick leave among full-time workers," Journal of Rural Health (2022): 1–10, 6.
- Henning-Smith et al., “Rural-urban differences in access,” 5.
- Henning-Smith et al., “Rural-urban differences in access,” 6–7.
- Our original data analysis of the 2017-2018 American Time Use Survey Leave and Job Flexibilities Module (ATUS) and the 2019 National Health Interview Survey (NHIS) codes individual respondents to non-metropolitan (used interchangeably with “rural”) and metropolitan counties. NHIS uses counties (specifically the 2013 NCHS Urban-Rural Classification Scheme derived from the Office of Management and Budget classification system) and ATUS uses a metropolitan/non-metropolitan statistical area classification, which is also done at the county level. We used the data within the survey to identify access and experiences among subgroups of interest (e.g., poverty level, race/ethnicity).
- PerryUndem and Bellwether Research survey commissioned for the National Partnership for Women & Families, Voters' Views on Paid Family + Medical Leave: Findings from a National Survey (Washington, DC, 2018), www.nationalpartnership.org/2018poll.