Appendix
New America is a “think and action” tank that is dedicated to realizing the promise of America in an era of rapid technological and social change. Within New America, multiple programs focus on issues related to family and economic security and well-being, including access to early care and education programs for families with young children.
New America’s Early and Elementary Education Policy team works to help ensure that all children, including young children with disabilities and developmental delays, have access to high-quality early learning opportunities starting at birth that prepare them to thrive in school and life. We aim to help realize this new system by conducting policy research and analysis, putting forth innovative policy recommendations, and disseminating new ideas to a variety of audiences, including federal and state policymakers.
The New Practice Lab’s theory of change centers on listening to the people who are most impacted by public programs: the people who they are meant to serve, and the people who deliver them. Our portfolio includes programs that support the family unit, working parents, and their children: tax credits, paid leave, and early education and child care. We believe that by bridging the gap between policy design and implementation, we can create a feedback loop that will help more families now—and create the conditions for more usable services and programs going forward.
Together, we embarked on an eight-week discovery sprint to better understand the barriers to early intervention that could lead to service gaps among high-risk children who may be missing out on important services, even when factors such as very low birth weight or low gestational age may make them automatically eligible.
Our team was curious to learn more about procedures for automatically connecting eligible babies to early intervention services, and to better understand provider, administrator, and family perspectives on what’s working well and what’s not. We were also interested in determining how widespread practices may be across hospital systems and geographies, and the extent to which learning and solutions may transfer across localities.
Methodology
Our discovery research primarily consisted of three lanes of effort:
- Learning more about current practices, gaps, and drivers by reviewing academic literature and other documentation about high-risk infants, their families, and their treatment and service transitions through their early years;
- Analyzing publicly available data about early intervention and related early childhood programs related to prenatal care, NICU stays, and perinatal care for high-risk infants; and
- Conducting 14 interviews with experts in the fields of neonatology, public policy, early intervention, social work, and perinatal health.
We did not engage with families directly at this point due to the time-limited nature of this discovery sprint and additional capacity requirements for conducting trauma-informed research with this population. To collect an initial reading of these perspectives, we relied on the perspectives of expert interview subjects in our third workstream, reviewed qualitative research describing family perspectives, and read postings on parent message boards.
What Is Early Intervention, and How Do Families Enroll?
Early intervention is an important and much-used program in the suite of federally supported early childhood services. Among the “core four” program areas identified in a previous brief, early intervention served 441,515 children in 2023, though this likely reflects a limited “point in time” count and not the full number of infants and toddlers who receive service in a year. This is better reflected by a cumulative count, such as the one provided by a birth cohort study conducted by the Infant and Toddler Coordinators Association.
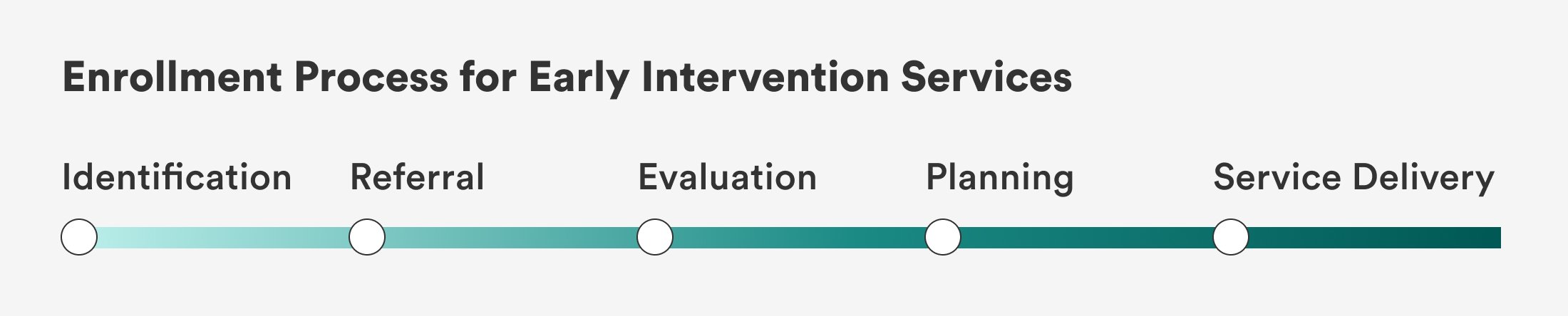
Many of the best-known federal programs such as Head Start, child care subsidies, and Women, Infant, and Children (WIC), are “means tested,” meaning there are income limits governing who can apply. Unlike means-tested programs, enrollment in early intervention (EI) services requires several steps: (1) identification via Child Find, (2) referral, (3) evaluation, (4) service planning, and (5) service delivery.
There are several considerations:
- Each step has its own set of federally mandated requirements that are then implemented at the state level in different ways.
- We do not exhaustively describe each step of the early intervention process here, but we explain the general pathway to enrollment along with potential pain points in each step to highlight why automatic eligibility and enrollment are important tools for families and providers.
- Finally, racial, demographic, and geographic disparities in access to health care persist and are woven throughout each step of the early intervention process, with significant impacts. Solving for these access disparities must remain a research priority to get the best outcomes for children and families who face the biggest barriers to help that they are entitled to receive.
Identification
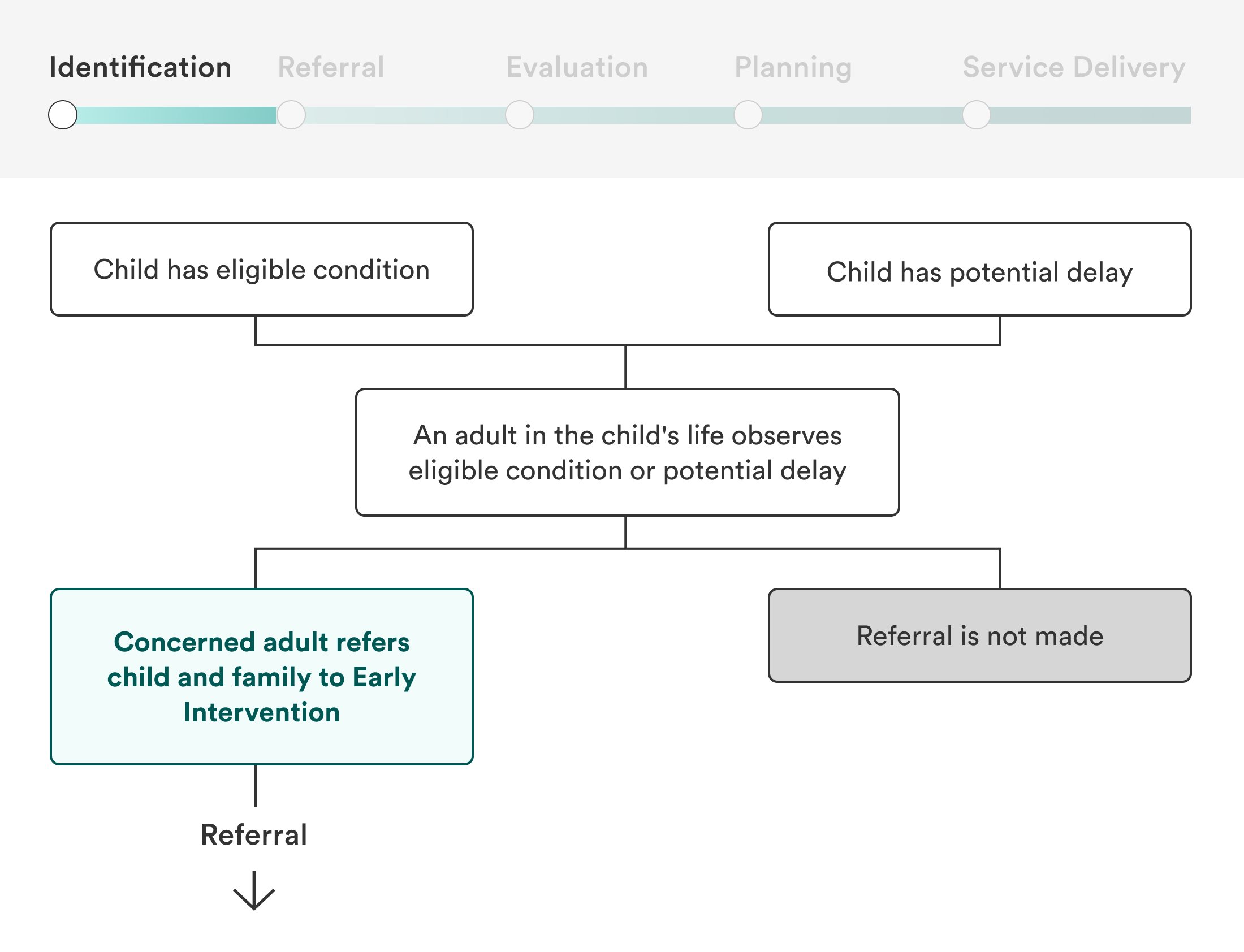
In the Child Find identification process required by IDEA Part C, children are eligible if they are under the age of three and have either observed developmental delays or eligible conditions with a high probability of developmental delay.
Even though infants are eligible, many are not identified for referral until they are 18 months or older. While some younger babies are diagnosed with delay or conditions very early and are quickly identified in Child Find, others have undiagnosed conditions that are difficult to pinpoint and will not be identified until later.
Preterm birth and low birth weight are easily observable characteristics that are strongly associated with risk of developmental delay. Many states allow them as eligible conditions, meaning their families can bypass more difficult steps to enroll. In states where this is not allowed, preterm and low birth weight babies will not be flagged during the Child Find process unless they have other eligible conditions.
Referral
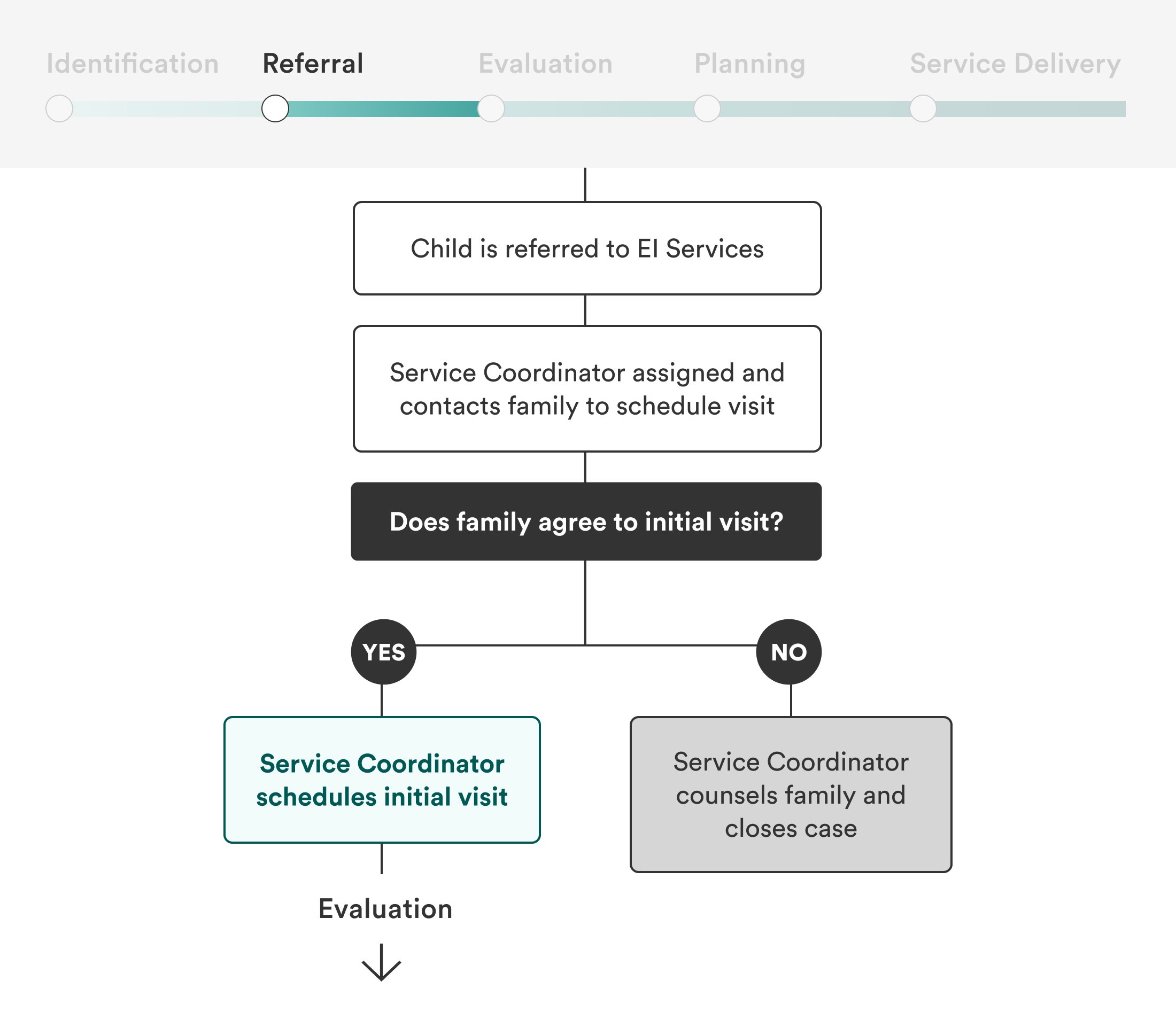
Anyone can refer infants and toddlers to early intervention services. For babies in the NICU, referrals are often dependent upon a doctor, social worker, or other hospital member providing information to families. Pediatricians who see NICU babies following hospital discharge can also make referrals. Once babies leave the hospital setting for the first time, however, referrals become more challenging and less likely, as qualifying presentations can become more subtle and difficult to diagnose.
Referral processes vary widely by state, county, and hospital, and understandings of referral criteria may vary even more. A misconception persists among medical providers and early educators that a child must already have a developmental delay in order to qualify for early intervention, when in fact children with certain medical conditions qualify simply with “high probability of resulting in developmental delay.”
When referrals based on low birth weight or prematurity are allowed but do not happen, families and infants lose time to access important services in the earliest possible stages of children’s development. Families who have not received appropriate information about their children’s conditions and the availability of services may not agree to an initial visit.
Evaluation
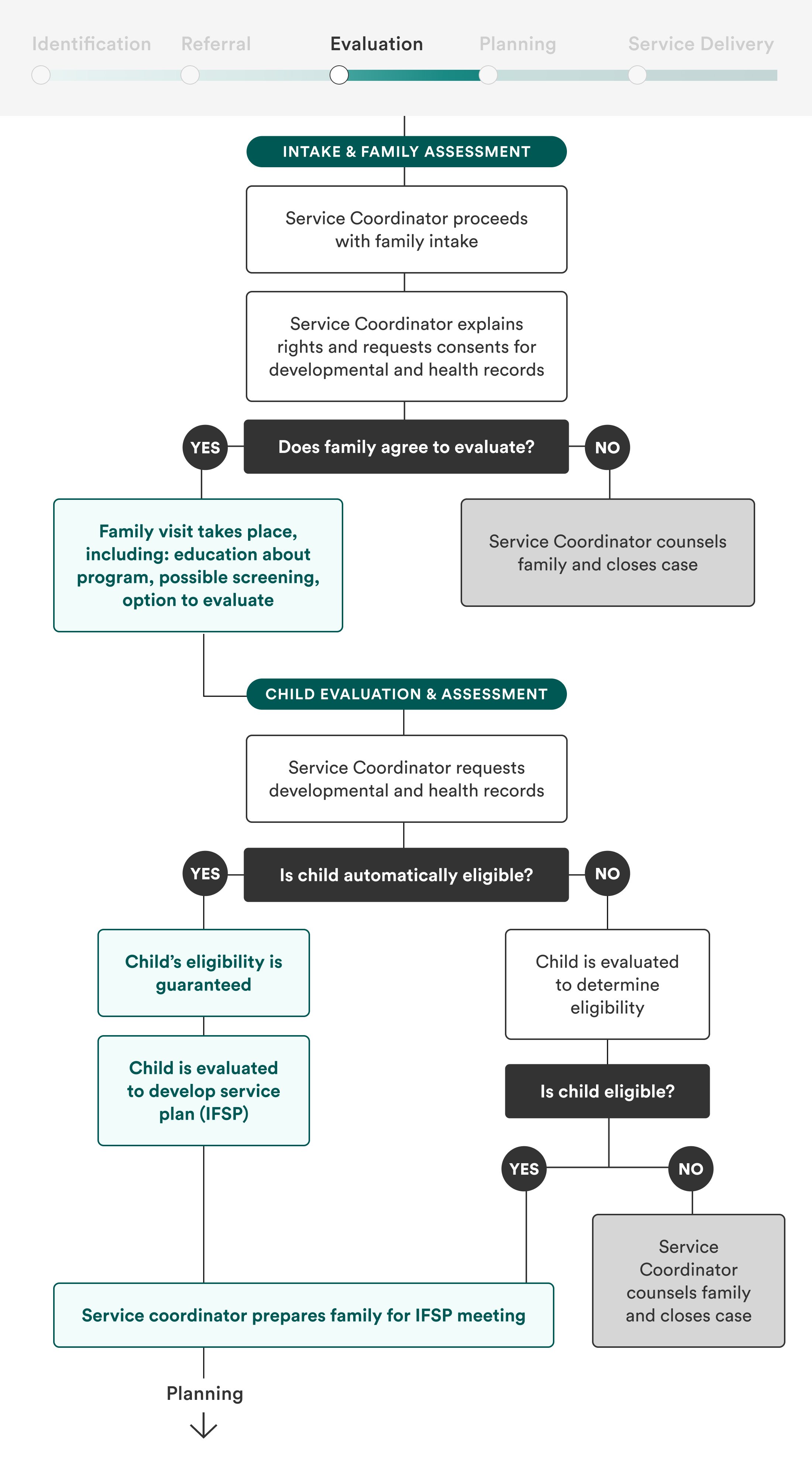
After being referred, the baby and their family must be evaluated further, including a meeting with the family to assess their routines, home environment, and developmental concerns, as well as an evaluation of the child’s developmental milestones. It’s a process that requires time, effort, and skill on behalf of the evaluators, and one that can be complicated by parental hesitation, stigma, language barriers, transportation barriers, and more factors.
Infants and toddlers that were not immediately identified and referred must first be evaluated by a specialist in order to be eligible, a process that can take weeks—a significant amount of time in a young child’s life. Evaluation services may be scarce and inconvenient for families to access.
To properly connect infants with appropriate therapies, evaluation will need to occur whether infants are automatically eligible for services or not. However, automatic eligibility for low birth weight and preterm infants exiting NICU will counterbalance the time-consuming and potentially stressful experience of evaluation with a guarantee of services.
Planning
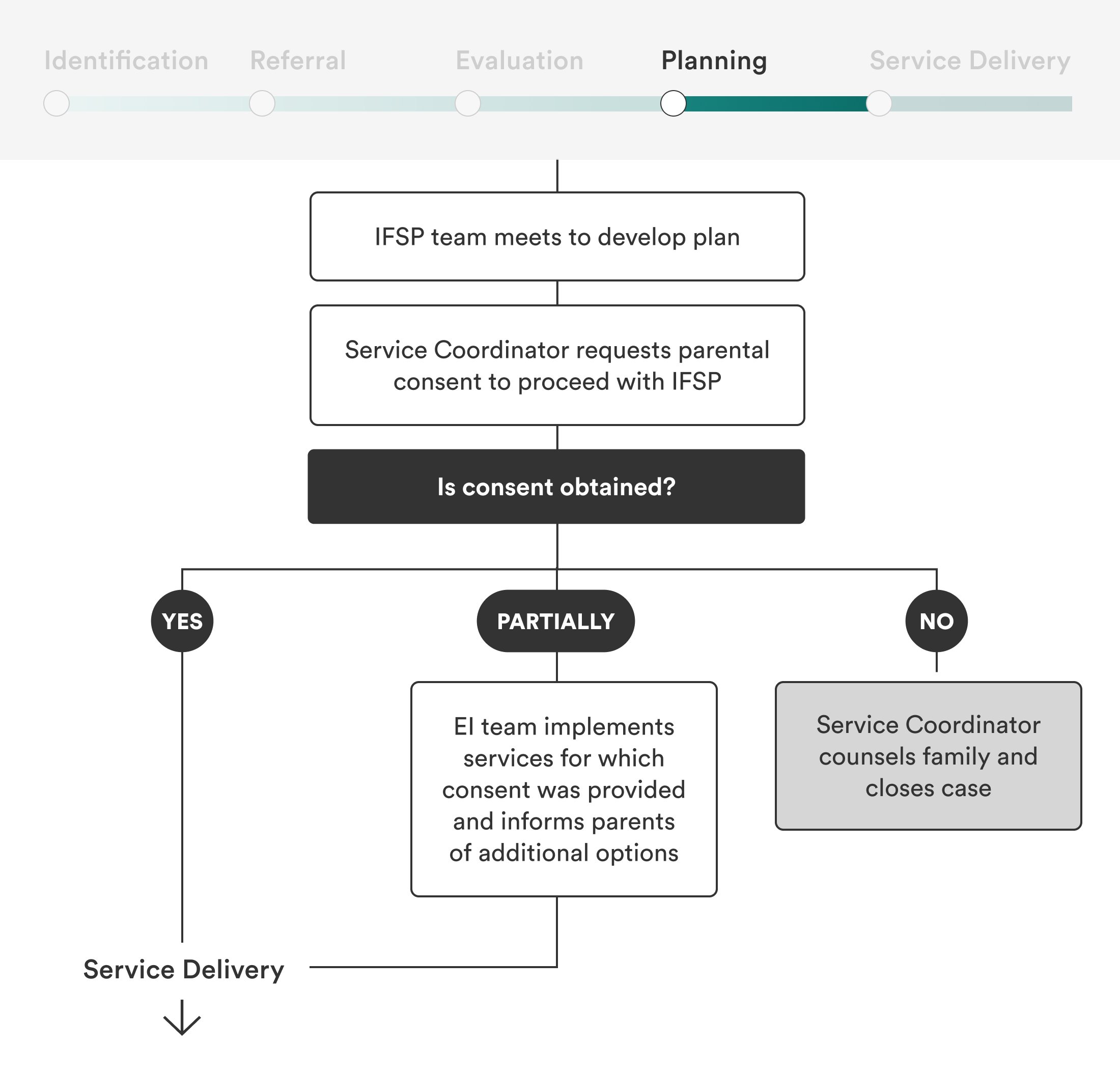
The early intervention team and family collaboratively develop a roadmap for services to support the child’s development known as an Individualized Family Service Plan (IFSP). The plans should include parent priorities, functional outcomes, appropriate services, and timelines for service. Once the IFSP is in place and consent is obtained, services can commence.
IFSPs are important (and required!) documents for coordinating early intervention services and will need to be in place whether or not a child is automatically eligible for services. Even though preterm and low birth weight infants will likely need some of the same early intervention services and may have even received some in NICU (speech therapy for feeding, for example, is common), their needs will vary and services should be targeted to meet families where they are. Since IFSPs are reevaluated annually, the longer infants are in the program, the more opportunities there will be to reassess and tweak service plans as needed.
Service Delivery
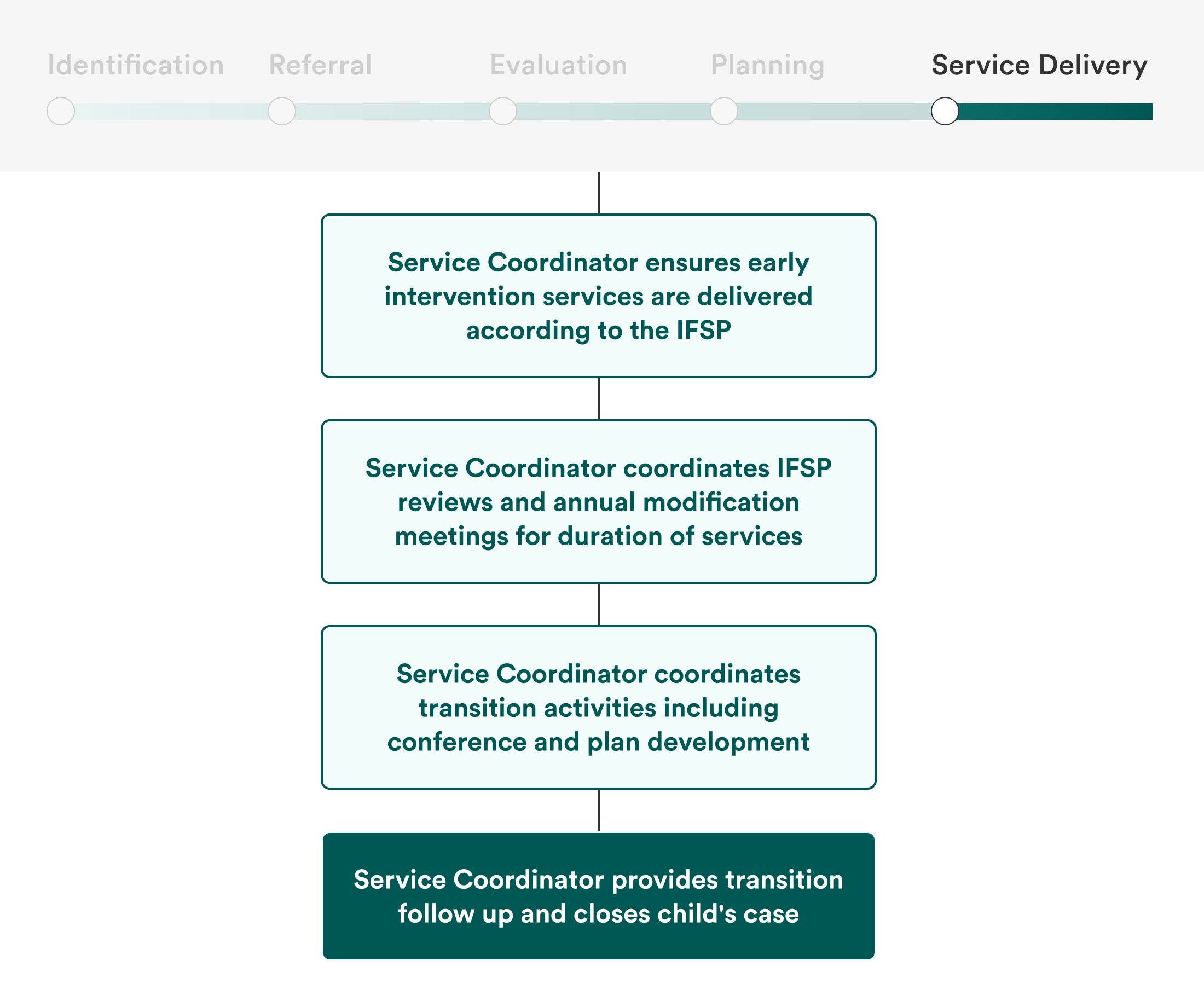
Once approved for services, families will need to be connected to appropriate provider such as occupational, speech and language, and physical therapists.
Automatic eligibility can enroll families more quickly, which is crucial for the populations that this approach would cover. Yet even with the advantage of an expedited process through automatic eligibility, the early intervention workforce shortage across the United States may make it difficult for families to find available providers. Furthermore, families with infants and toddlers have limited time and energy. Lower-income families lack cash and basic needs like food, diapers, housing, and reliable transportation, and may have demanding or irregular work schedules, language barriers, or other challenges that make it difficult to attend appointments consistently. Policies must address the chronic early intervention workforce shortage and the overall accessibility of early intervention programs in order to more comprehensively improve the system.
