
Table of Contents
- Executive Summary
- Introduction
- I. Providing Care Can Shape Men’s Attitudes and Beliefs
- II. Men Who Care
- III. Men and Work-Family Conflict: The Heavy Toll on Men who are High-Intensity Caregivers and/or Parents
- IV. An Overwhelming Majority of Men Value Care and Believe it Should be Equally Shared. But Belief Isn’t Associated with Practice.
- Conclusion
- Methodology
Introduction
I hear and I forget
I see and I remember
I do and I understand
– Confucius
When the COVID-19 pandemic forced his workplace to shut down and his managers to lay him and other staff off in March 2020, Ronald Taylor, an occupational therapist in Portland, Ore., became the primary carer for his two daughters, ages 5 and 8, whose schools had also shut down. His wife, Kerala, a marketing and strategic planner, was able to work remotely and keep the family afloat financially. For weeks, Ronald was with his children 10 hours a day, 7 days a week and in charge of the home front.
While some men in similar situations—during the pandemic and in the Great Recession of 2008—may have felt out of their depth, for Taylor, “it was wonderful in many ways.” But that’s because the experience of hands-on care was not new. When his eldest daughter was born, he stayed home caring for her for 15 months because his wife earned more money and the couple couldn’t afford childcare if they both worked. “It changed me as a person,” he said.
Taylor was a paramedic for six years. He has a graduate degree. He’s the only Black male hand therapist in the state of Oregon. “And the hardest job I’ve ever had was taking care of my baby daughter for 10 hours a day,” he said. “Most men don’t have any idea what that’s like, or what their wives are going through. They think, ‘I went to work, I worked hard.’ I want to tell them, ‘Yeah, she worked harder.’ And unless you have that experience, you think paid work is more important than taking care of another human being.”
Taylor remembers taking his baby daughter out in her stroller one day. He walked by a construction site. “I just felt so ridiculous,” he said. “I’m supposed to be a man, and I’m pushing this baby stroller while my wife works. This one guy asked me, ‘Oh, you’re just taking care of your baby, huh?’ I said, ‘Yeah, but I wish I was doing what you’re doing.’ And then the guy said, ‘I wish I was doing what you’re doing.’”
As he reflected on this pivotal moment in his life, Taylor paused. “I think if we could do it more, and it was respected in society, I think a lot more men would like to be around their kids more,” he said. “But I don’t think it’s something society values.”
In 2020, an unprecedented pandemic has upended daily life around the globe. Never before has the central role that care plays in our lives been made more clear as families struggle with work and care responsibilities in the face of school closures and childcare shutdowns while contending with the needs of isolated and aging parents, illness, fear, and even death.
Women and mothers, who are still culturally expected to be primary carers, typically spent about twice the amount of time giving care before the pandemic. During the upheaval, as schools and childcare facilities have shut down or reduced in-person attendance, women have taken on the bulk of the expanded load of care work and homeschooling and are paying the price—cutting back on work hours or dropping out of the workforce entirely at higher rates than men, and experiencing high rates of stress, anxiety, and sleeplessness. Some academics and advocates worry women will be set back a generation.
… women have taken on the bulk of the expanded load of care work and home schooling, and are paying the price.
Yet, in a phenomenon that bears close attention, the lives of men like Taylor have also changed dramatically. Nearly overnight, an enormous number of white-collar men who were accustomed to being rewarded for working long hours in offices, often reached after lengthy commutes, began working remotely. In-home offices, at kitchen tables, in laundry rooms, and many with children underfoot. More than three-quarters of essential healthcare workers are women. They’ve been forced to work long hours in the pandemic and are simply unable to be the primary carers at home. It remains to be seen whether their male partners will have been forced to step up and take on more care responsibilities. (One study using survey and interview data with mothers of young children in the early weeks of the pandemic found that some front-line health workers relied on extended family stepping in to help with childcare rather than on their spouse or partner.)
Unemployment and furloughs have been more severe for women and women of color in this pandemic because they’re overrepresented in the service and hospitality industries that have been hit hardest. But millions of men have also lost jobs and livelihoods—more than 20 million people in the United States were unemployed in May 2020 at the height of the pandemic-related shutdowns, and 11 million people remained out of work in October 2020—disrupting gendered patterns of work and care. Research conducted at the height of the first wave of the pandemic found that while women were doing more care work and homeschooling than men, men were still doing far more care work than they had before the pandemic, leading, in some families, to more equal sharing of care and domestic labor.
So the question is: will the experience of doing more hands-on care—or, at a minimum, the day-to-day exposure to just how much work it takes to give care and run a household—change men’s attitudes, beliefs, and behaviors? Will men, for so long defined by the gendered expectation of being primary breadwinners and a family’s financial provider, remain more active carers once the pandemic ends? Will they, like Taylor, become changed by this experience of care? And will that lead to healthier children and families, as research suggests, and to fairer divisions of work and care that could finally push forward the journey toward gender equality that’s been stalled for decades?
Will men, for so long defined by the gendered expectation of being primary breadwinners and a family’s financial provider, remain more active carers once the pandemic ends?
Previous studies on whether men’s experience of providing care changes their attitudes and behaviors are mixed. Some have found that men’s involvement in household labor is often “situational,” meaning they’ll pitch in or take over when they have no other choice. For instance, men whose wives work opposite schedules from them or who work evening shifts and are home with the kids during the day tend to do more at home, whether they believe in gender equality or not. It’s just what they have to do—a phenomenon that lawyer and work-life scholar Joan C. Williams describes as blue-collar men and fathers “walking the walk” of gender equality, even if they don’t talk the talk. For white-collar men, it’s often the opposite, she found—they say they believe in gender equality, though they’re in more traditional partnerships and divisions of labor, largely because of the expectation of long work hours for white-collar jobs. And men in heterosexual couples who telecommuted before the pandemic tended to pitch in more with child care and housework only if their partner or spouse worked full-time.
Yet when men lost jobs in the Great Recession of 2008 and took on more household and care work at home, researchers found that many began to move away from the breadwinner identity to find meaning as active, engaged fathers.
Throughout much of the twentieth century, academics all but ignored men as carers, seeing their role in the home as “irrelevant.” Even when women began entering the workforce en masse in the 1970s, change has been slow in the cultural expectation that care work is “women’s work.” Not long after Wade Horn, assistant secretary for children and families at the Department of Health and Human Services under President George H.W. Bush, said that men being involved in care work was “nonsense,” sociologist Scott Coltrane released a groundbreaking qualitative study on men and care. He reported that men were “transformed” by their experience of care work, with fathers developing increased sensitivity to their children, their families, and the difficult, time consuming, and yet profoundly meaningful work of care and connection. In other research, fathers of children with special needs have reported that their experiences providing care increased their patience, empathy, tenderness, and humility.
Already, intriguing research is emerging about how men’s roles in care work are evolving during the pandemic. One survey of Australian families under lockdown in May 2020 found that, with schools and childcare closed, the domestic load of unpaid work rose for both men and women, though women took on a greater share of the responsibility. Still, men began spending about as much time providing care during the pandemic as women had pre-pandemic, narrowing the relative gender gap in time spent on childcare from 52 percent to 41 percent. Another study, based on a U.S. sample, similarly found that 10 to 15 percent of the different-sex couples studied had moved toward a more equal division of unpaid caring and housework in the pandemic.
Our quantitative survey sheds important new light on who men who give care are and shows how much they do, how they, too, struggle with work-family conflict, and that men who are High-Intensity Caregivers and/or Parents, HICP, have been forced to reduce hours or drop out of the workforce at rates similar to HICP women. And the perspectives shared in our qualitative research, in addition to previous research, suggest that men’s lives can be profoundly transformed by the experience of giving care. The men in our focus group discussions repeatedly said that while care work can be exhausting, emotionally draining, stressful, and lead to burnout, it is also deeply meaningful. Their names have been changed to protect their identities, except in cases where they’ve permitted us to use their identities and comments.
James, 49, from Florida, is one of our focus group members with experience caring for an adult. He cares for his mother, administering medicine, handling her finances, driving her to medical appointments, and doing all he can to keep her living independently at home and out of assisted living or a nursing home. “It is time consuming,” he told us. “But it is worth it.”
Indeed, research on men who’ve taken paid family leave to spend time caring for loved ones shows the experience can have deep, long-lasting impacts on the health and wellbeing of men and their relationships with their partners, their families, and their children. In many countries, men who’ve taken paid leave wind up becoming more engaged and active in their children’s lives over the long term. They even live longer. And yet one study in Spain found that men who took paid leave to care for an infant were less likely to want any more children. Possibly, the researchers surmised, “due to their increased awareness of the costs of child-rearing.”
When it comes to women in the workplace, there are rafts of research studies, surveys, employee resource groups, special programs, task force studies, recommendations, and self-help books. But we know very little about men and their experience as carers.
Building on the emerging work of academics, the Pew Research Center, Boston College Center for Work and Family, Promundo, and others, the Better Life Lab sought to help fill in some of the blanks on men and care with a nationally representative survey, in partnership with NORC at the University of Chicago, and a series of online focus groups and additional qualitative reporting. In this report, one in a series using our data on men and care, we provide a clearer picture of what we know about men who give care—who they are, what they do, and how they think about it. And we probe the question of how their exposure to giving care impacts their lives, attitudes, behaviors, and those around them.
Although the data was collected before the global pandemic, it can serve as both a baseline to measure change as well as a useful guide in understanding men’s experience providing care, the channels that enable them to do it, the barriers that keep them from it, and the lasting impact men’s caregiving may have in the future.
Terminology
High-Intensity Caregivers and/or Parents: In analyzing our survey data, we initially planned to analyze and compare the experiences of three groups of men: men who care for adults, fathers, and men who are not caregivers. However, it quickly became clear that a significant number of respondents have both provided care for an adult family member or close friend, and are, at the same time, parents who have cared for a child under 18 with a medical or behavioral condition or disability (special needs.) In our survey, 60 percent of parents who have cared for children with special needs have also cared for an adult. Conversely, nearly one-third of those who have cared for an adult are also parents who have cared for children with special needs. And across 27 comparisons, we found only three statistically significant differences in attitudes between those who care for adults, parents who care for children with special needs, and those who fall into both categories. For these reasons—because there is so much overlap in actual people and because of the similarities in attitudes—we chose to group these adults together as High-Intensity Caregivers and/or Parents, abbreviated in this report as HICP.
We compared the experiences and attitudes of those in the HICP group to parents who have never cared for a child with special needs, a group we labeled Other Parents (or Other Fathers, when discussing men exclusively.) We compared both of these groups of caregiving adults with those who have never provided care, a group we called Non-Caregivers. To increase our understanding of men’s experiences with caregiving, some of our analyses compared these three groups while looking only at men, while for other questions, we compared men in the HICP or Other Parent group to women in these groups.
Caregiving: The word “caregiving” means different things to different people, and even is defined differently in national surveys conducted by different organizations. For some, it encompasses a wide variety of caring activities—parenting, caring for an adult, self-care, paid and unpaid care work—on behalf of a variety of people. Others define the word narrowly. For instance, federal legislation and some advocacy organizations refer to “family caregivers” as adult family members or others and who provide ongoing assistance to people with a “chronic or other health condition, disability, or functional limitation.” For the purposes of this report, we use the term “caregiving” to refer to a broad range of care tasks and responsibilities, including hands-on and hands-off care and parenting. Thus, we also refer to two of our three groups—the HICP and Other Parent groups—as “caregiver” groups, because individuals in both these groups perform the broad range of care tasks and responsibilities that we consider to be caregiving.
Previous research has also found differences and “unique stressors” in the experience of fathers who have provided care to a child with special needs compared to fathers who have never cared for a child with special needs. About one in five children under 18 require special accommodations or services due to a chronic physical, developmental, behavioral, or emotional condition, and about two-thirds of these children require comprehensive services in addition to medication, according to the U.S. Department of Health and Human Services. These additional needs can be challenging, overwhelming, and stressful for parents. Research shows that in addition to higher levels of marital stress and lower relationship satisfaction, fathers of children with special needs experience greater child-related stress than other fathers. And because children with special needs can require specific routines or support structures, parents, and fathers in particular, may find it more difficult to manage care responsibilities with work demands.
We found that, even before COVID-19, men said they were doing much more care work than they are often given credit for—by their partners, families, their workplaces, by policymakers, in the national conversation, and even in their own minds. Though it’s important to note we asked about providing specific care tasks, not the frequency or duration of performing them, and that some studies have found men often think they’re doing a larger share of care work than women think they are. We found that some men’s limited view of what providing care means, in addition to the still-powerful biased traditional belief that men are suited to breadwinning and women to care work, are part of what keeps men from providing care. But those are not the only barriers. There are also structural, cultural, and financial obstacles that push men into breadwinning roles, making it far less likely and far more difficult for men to actively choose to provide care if they wish.
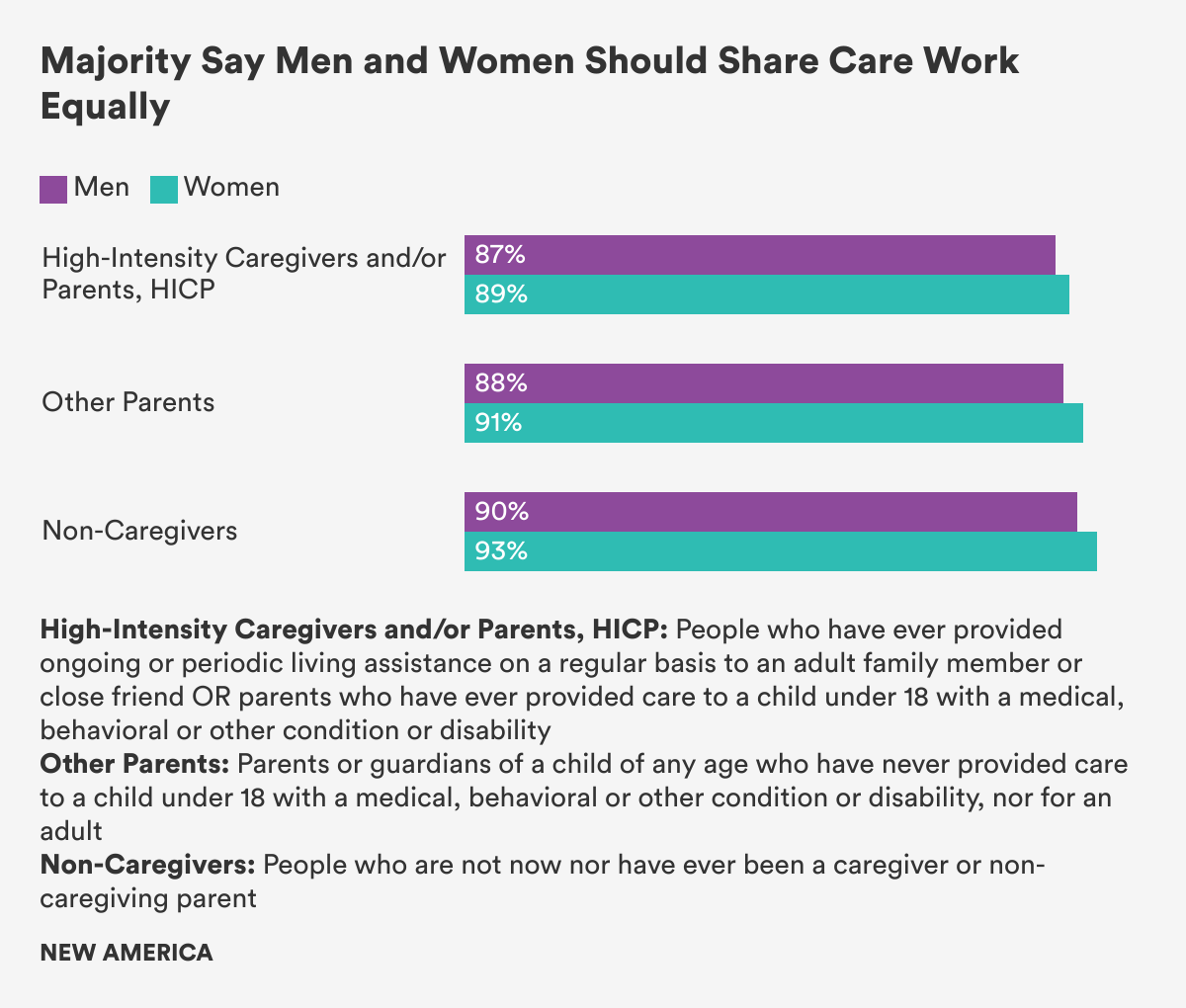
And, as other studies have, we found a wide gulf between what men say is ideal and what they actually do. For instance, 91 percent of our respondents said that care responsibilities should be equally shared between men and women, and men in all groups overwhelmingly said men and women should share care responsibilities equally. Yet when a family member is ill, has a disability, or needs long term care, 45 percent of our respondents said the responsibilities mainly fall on women. (46 percent said the responsibilities are divided about equally. Just 4 percent said they fall mainly on men.)
Figure 1
Often, we found men’s care work happens under the radar in a way that would hide their care in formal surveys or from public view. For instance, rather than use formal work-family supportive policies as many women do, many men were able to use the flexibility that comes from being in a position of power or privilege. George Smith, one of our focus group members who agreed to let us use his full name, is a financial planner, father of four, and primary carer for his ailing 77-year-old mother. Yet he’s never officially taken paid family leave for care, even when his mother was in the hospital for nearly two months. Instead, he uses paid sick and vacation time when he needs to and works a remote, flexible schedule in order to care for her. “I just incorporate it into my paid time,” he said.
Our initial question, as we began to analyze the survey data, was whether the experience of providing care would be associated with men valuing it more. Or conversely, if they believed care work was valuable, whether that belief would be associated with providing care. We didn’t find that. Instead, we found that men, by and large, say they do value care, whether or not they have ever provided care to loved ones. But that theoretical valuing of care doesn’t translate into their actually doing it. Rather, our focus groups and interviews suggest that when men actually do give care, the experience can be life-changing.
Men, by and large, say they do value care, whether or not they have ever provided care to loved ones… when men actually do give care, the experience can be life changing.
So the real question is, if men do value care, and express a preference for more equally sharing care responsibilities, what is keeping them from having that potentially transformative experience and being as engaged in care work as they would like? And what needs to change for that to happen? Our data suggest that transforming work culture, family-supportive policy, and gender norms to recognize that workers of all genders have care responsibilities is key to creating space for men to give care and to making the lasting social change that will increase equity and benefit the health and wellbeing of men, women, children, families, and ultimately all of the economy and society.