
Automatic Eligibility for High-Risk Infants
One way to potentially close the service gap to babies is through policies offering automatic eligibility and enrollment—in other words, focusing attention not just on infants and toddlers already diagnosed with delays and disabilities, but on those at especially high risk of developing them as well. By identifying and connecting these babies and their families to early intervention services based on risk factors rather than diagnosed delay, states can potentially reduce the friction of the typical program enrollment process for families, enabling proactive service delivery and getting eyes on infants’ development instead of waiting for them to struggle.
Current Eligibility Pathways
For the purposes of delivering early intervention services under the Individuals with Disabilities Education Act (IDEA), states independently determine (1) what constitutes an eligible disability or delay, (2) what conditions put infants and toddlers at risk of developing disability or delay, and (3) other high-risk factors.1
Delays are usually expressed as a percentage to estimate the degree to which a child’s development differs from norms based on chronological age. These metrics vary widely from state to state, both in terms of the percentage of delay required to qualify for services and the number of delays that are present. For example, a child with a 25 percent delay in speech may qualify for services in one state, but not in a state that requires a 33 percent or 50 percent delay (see Table 1). Being diagnosed with any level of delay can be a journey in itself.
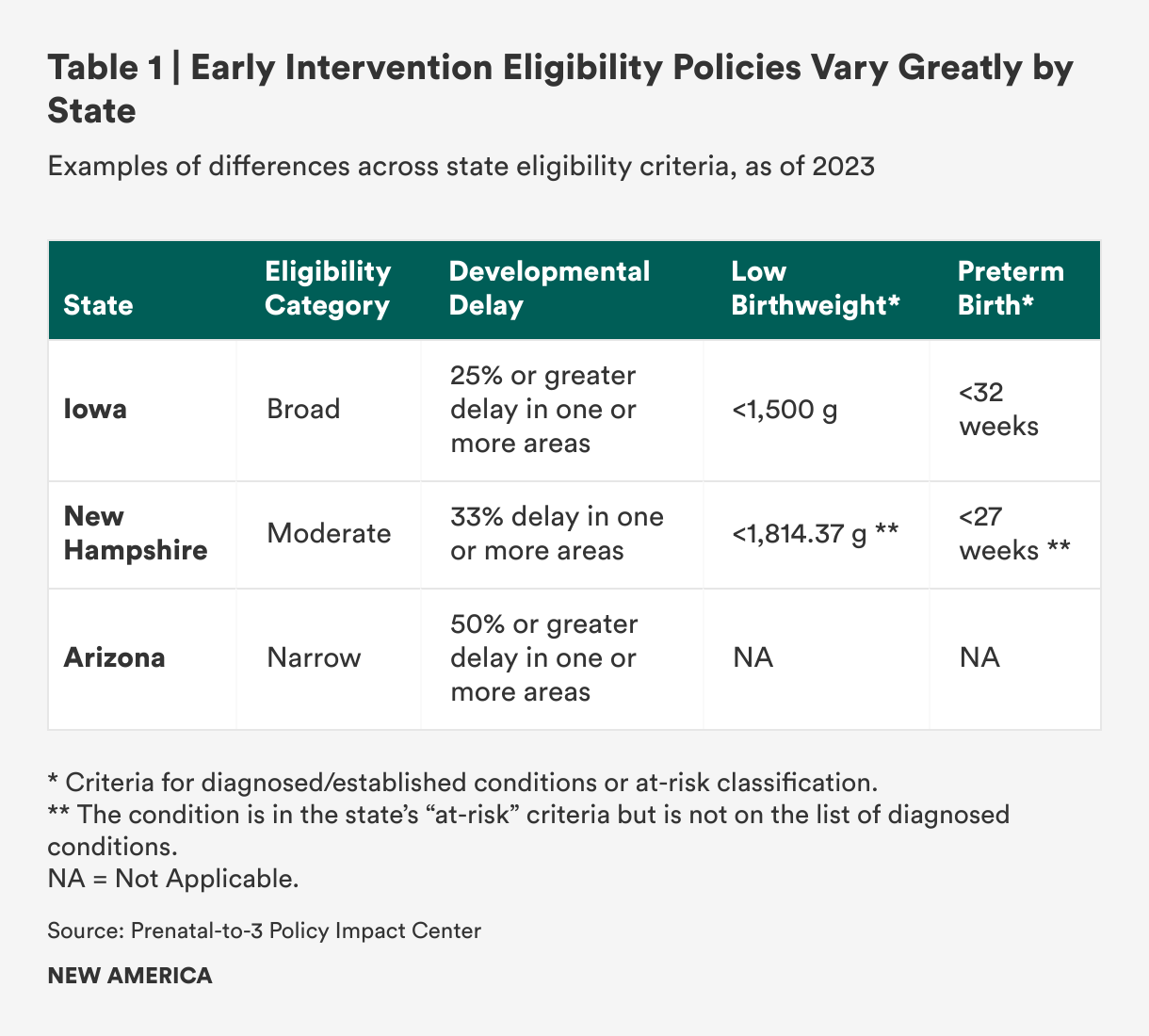
For cases where delays are not yet observed but are likely, lists of eligible diagnosed conditions exist. Many are specific conditions like hearing impairment, trisomies, and spina bifida, and these lists can be lengthy and detailed: One study identified over 600 diagnosed conditions across all state lists.2 Some state lists include risk factors covering health and environmental conditions at birth: babies born at low gestational age or very or extremely low birth weight, with neonatal abstinence syndrome or born to a parent with substance use disorder, or who are experiencing homelessness or have child welfare involvement.3 In those states, these conditions—either alone or in conjunction with other conditions—qualify infants as eligible for early intervention.
In general, the need for eligibility policy that is both evidence-based and better aligned across states has been noted by researchers and advocates, but as of now, state variation stands. According to a comprehensive study on states’ eligibility criteria, “despite challenges related to diagnosed conditions, currently states have an OSEP [Office of Special Education Policy]-approved policy regarding their eligibility criteria and are in full compliance with the law, with no requirement for state lists to be based on scientific evidence or otherwise empirically justified.”4
Implementing Automatic Eligibility
Determining eligibility can be time-consuming when it involves waiting for infants and toddlers to miss expected milestones. But, automatic eligibility for early intervention is allowed when a child under the age of three has been diagnosed with a condition that indicates a high probability of delay. Automatic eligibility theoretically allows families of babies with qualifying conditions to bypass complicated determinations and processes, enabling families to start receiving services more quickly. This may be easier to implement for some conditions than others; statistics like very or extremely low birth weight and low gestational age are consistently captured at birth and can be verified through medical records. Importantly, most babies with either or both of those two risk factors are often served in neonatal intensive care units (NICUs) for substantial lengths of time, providing a common touchpoint for connection to services for the babies who may need them.5
Connecting families of low birth weight and preterm babies with early intervention services through the NICU is a promising delivery opportunity. All but 15 states include low birth weight, preterm birth, or both as eligible conditions to qualify for early intervention. Both characteristics are strong predictors of future need for these services, and their prevalence is high in the United States. More than 10 percent of all U.S. babies are born preterm, and most of these infants spend time in NICU. Nearly 9 percent of U.S. babies have a low birth weight, and those with certain health conditions are also likely to be admitted to the NICU. Preterm infants face increased risks of conditions such as cerebral palsy, autism, and attention-deficit hyperactivity disorder.
Connecting families to services through NICU is an established best practice in physical, speech and language, and occupational therapy professions, but also a matter of increasing urgency and potential impact. Medical advancements have resulted in babies born at progressively earlier gestational ages who are able to live and grow. At the same time, high-risk births are all too common as prenatal health care and prevention programs in the United States lag behind many developed countries. The March of Dimes has identified a number of factors that increase the number of preterm infants who are born at risk of developmental delays and disabilities: lack of supportive policies like paid family and medical leave, the prevalence of unhealthy environments, and barriers to primary care to prevent and manage chronic conditions. The growing number of preterm births makes the early identification and enrollment of eligible infants through automatic eligibility even more critical.
Successfully using automatic eligibility to bring early intervention to high-risk infants in the NICU may also help address known disparities in access. Black, American Indian or Alaska Native, and Native Hawaiian or other Pacific Islander mothers are more likely to have preterm and low birthweight infants compared to white mothers, but are also less likely to be served by early intervention services than those of all other races and ethnicities.6 Children from families with lower incomes are 26 percent less likely to receive a developmental screening than children from higher-income families.7 By prioritizing preterm and low birth weight babies, it might be possible to move the needle on these gaps and provide more equitable service to children and families.
Good Policy Does Not Guarantee Successful Implementation
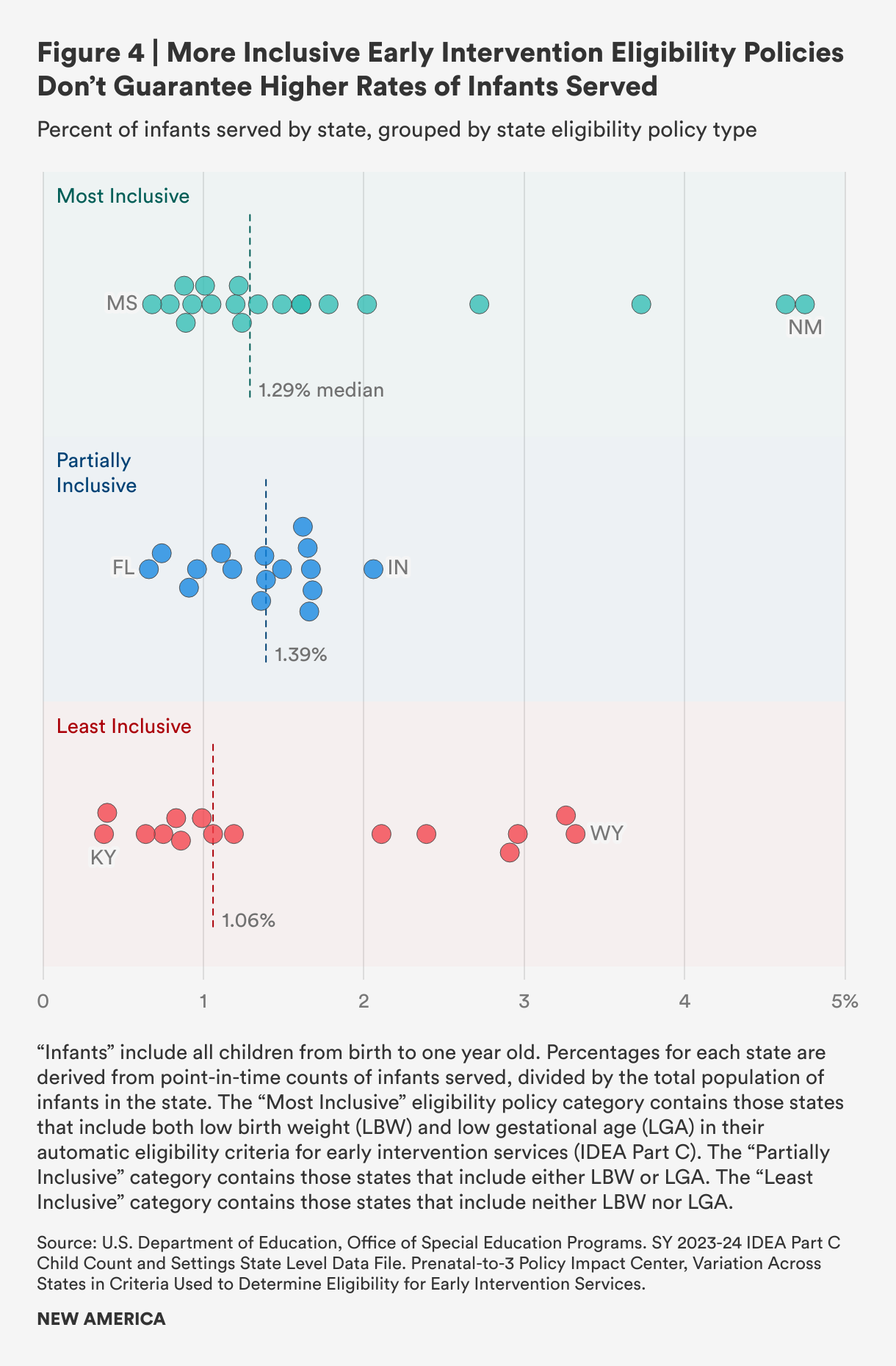
To gauge the potential effectiveness of automatic eligibility, we looked at state eligibility policies’ inclusion of low birth weight and low gestational age and categorized each as “most inclusive,” “partially inclusive,” or “least inclusive” across all 50 states and the District of Columbia.8 We looked for any correlation between inclusivity and the percentage of infants served according to program data (see Figure 4). We found that policies characterized as most inclusive did not necessarily correspond with a higher rate of infants served, while some states with least inclusive eligibility policies serve a relatively high percentage of infants. Our analysis shows that strong policies alone do not necessarily result in higher early intervention service rates for infants and their families, and we theorize that implementation challenges are likely a factor, along with longstanding underfunding.
Given the complexity of eligibility policies, our analysis is illustrative but not conclusive in drawing a line between eligibility policy for low birth weight and premature babies and service to infants. Future studies should further analyze the variability of eligibility criteria and their association with early intervention services rates, along with other variables such as funding. If serving more infants in early intervention is a goal, state leaders could use better information about where policies are working well to bring more infants into the system, and how these policies could be better implemented.
The factors influencing low rates of service to infants are complex, but whatever the reasons, the disconnect has implications for children and families who should qualify. A recent article in the Hechinger Report highlighted a case in Illinois where children who were eligible by state criteria were not connected with early intervention services.9 As a result, these children missed out on services that are designed to encourage their healthy development and long-term success that they are entitled to receive. This is not isolated: A 2017 study in an Oregon hospital found that 71.5 percent of low birth weight infants were not enrolled in early intervention services by their first high-risk infant follow-up appointment, and of those not enrolled, 42.1 percent would qualify for services due to high-risk conditions.10
While it is unclear how widespread the disconnect between automatic enrollment and service delivery is, either in Illinois or across the country, it represents an all-too-common problem: a strong policy to help families with young children that may not meet their needs because of flawed implementation.
Citations
- IDEA part C regulations include five categories of delay—physical, cognitive, communication, social or emotional, and adaptive—along with a non-exhaustive list of potentially eligible conditions: chromosomal abnormalities; genetic or congenital disorders; sensory impairments; inborn errors of metabolism; disorders reflecting disturbance of the development of the nervous system; congenital infections; severe attachment disorders; and disorders secondary to exposure to toxic substances, including fetal alcohol syndrome. See: “§ 303.21 Infant or Toddler with a Disability,” Code of Federal Regulations (2025), source.
- Brian Barger et al., “State Variability in Diagnosed Conditions for IDEA Part C Eligibility,” Infants and Young Children 32 (2019): 231–244, source.
- For simplicity throughout this report, we will use “low birth weight” for both very low (>1500 grams) and extremely low (>1000 grams) birth weight, and use “preterm” in lieu of “low gestational age,” typically defined as any birth before 37 weeks.
- Barger et al., “State Variability in Diagnosed Conditions for IDEA Part C Eligibility,” source.
- While national data is not readily available, one study found that 56.3 percent of preterm infants were low birthweight, and 72.4 percent of low birthweight infants were preterm, demonstrating some of the potential overlap between these two conditions. See: Stephanie A Leonard et al., “Associations Between Preterm Birth, Low Birthweight, and Postpartum Health in a Predominantly Hispanic WIC Population,” Nutrition Education and Behavior 46 (2014): 499–505, source.
- Latoya Hill et al., Racial Disparities in Maternal and Infant Health: Current Status and Efforts to Address Them (Kaiser Family Foundation, 2024), source; Office for Civil Rights, 45th Annual Report to Congress on the Implementation of the Individuals with Disabilities Education Act (Department of Education, 2023), source.
- LaRue Allen and Rebekah Hutton, eds., “Opportunity Gaps in Early Care and Education Experienced by Children from Birth to Pre-K,” in Closing the Opportunity Gap for Young Children (National Academies Press, 2023), source.
- “Variation Across States in Criteria Used to Determine Eligibility for Early Intervention Services,” Prenatal-to-3 Policy Impact Center, Vanderbilt University, source.
- Sarah Carr, “Parents of Premature Babies Struggle to Get Help Their Children Are Entitled To,” Hechinger Report, January 23, 2025, source.
- Kristi Atkins et al., “Part C Early Intervention Enrollment in Low Birth Weight Infants At-Risk for Developmental Delays,” Maternal and Child Health 21 (2017): 290–296, source.