Protecting Infant Health: Closing Early Intervention Service Gaps
Abstract
Early intervention services are an important federally funded program for families with children under three years of age who may be diagnosed with or are at risk of developmental delay or disability. The program’s impacts can be profound: Early intervention helps strengthen cognitive, motor, and language skills; reduces the likelihood of childhood maltreatment; and can lower education costs through reduced need for special education.
Unlike means-tested programs, any child with a developmental delay or disability is entitled to early intervention, but first they must be identified, referred, evaluated, connected to providers, and then served. Unfortunately, there are policy and implementation pain points at every step in the process that can block access. Only 53 percent of children who are referred end up enrolled, and rates of enrollment for children under the age of one are particularly grim. Policies like automatic eligibility for some high-risk infants, like those admitted to the neonatal intensive care unit (NICU) due to low birth weight or prematurity, are designed to better connect children to services, but even strong policies can be vexed by implementation challenges. The result is that these children and families can still fall through the cracks.
This descriptive report was generated following an eight-week “discovery sprint” conducted by New America’s Early Education and New Practice Lab teams that included a review of academic literature and documentation on high-risk infants, their families, and early-years service transitions, an analysis of publicly available data on eligibility policy and early intervention services to infants, and interviews with experts across neonatology, public policy, early intervention, social work, and perinatal health. We investigate the implementation challenges associated with the successful handoff of children exiting the NICU to early intervention services, and suggest strategies for serving more babies when they are automatically eligible.
Acknowledgments
This report would not have been possible without contributions from experts in neonatology, public policy, civic technology, early intervention, social work, and perinatal health, including but not limited to: Kayla Buswell Khan, vice president of the Kids Division at Northwest Center; neonatal nurse practitioner Alanna Dessouky; Elisabeth Wright Burak, senior fellow at the Georgetown University Center for Children and Families; and Matt Lee, attending neonatologist at Good Samaritan Hospital of Los Angeles, Santa Barbara Cottage Hospital, and Start Early.
Editorial disclosure: The views expressed in this report are solely those of the authors and do not reflect the views of New America, its staff, fellows, funders, or board of directors.
Downloads
The Value of Early Intervention for Infants and Toddlers
Early intervention services are an important federally funded program for families with children under three years of age who may be diagnosed with or are at risk of developmental delay or disability. Authorized in 1986 by Part C of the Individuals with Disabilities Education Act (IDEA), early intervention programs are run at the state level. They rely on a mix of federal and state funds to deliver therapeutic services to children and families who have been referred, evaluated, and approved for services based on state-determined criteria.
The purpose of early intervention is exactly what it sounds like: to intervene early to connect infants, toddlers, and their families with appropriate developmental supports before school entry. Early intervention helps infants and toddlers eat, sleep, move, speak, and play better, creating a strong foundation for the “free and appropriate public education” that IDEA guarantees. Early intervention uses a family-centered approach that takes into consideration a family’s environment, routines, and preferences, and integrates the family into services for children. When families can access the program, the impacts can be profound: Early intervention helps strengthen cognitive, motor, and language skills, reduces the likelihood of childhood maltreatment, and can lower education costs through reduced need for special education.
Early intervention provides critical support for the health and well-being of infants and toddlers, but delivery is challenging: Children with disabilities or delays, or at risk of developing delays, must be identified, referred, evaluated, and enrolled with an individualized family service plan before they can begin receiving services. Pain points at every step in the process interfere with access to early intervention.
The Government Accountability Office reported that 53 percent of the 650,211 children referred for early intervention services ultimately enrolled, expressed as real numbers in Figure 1.
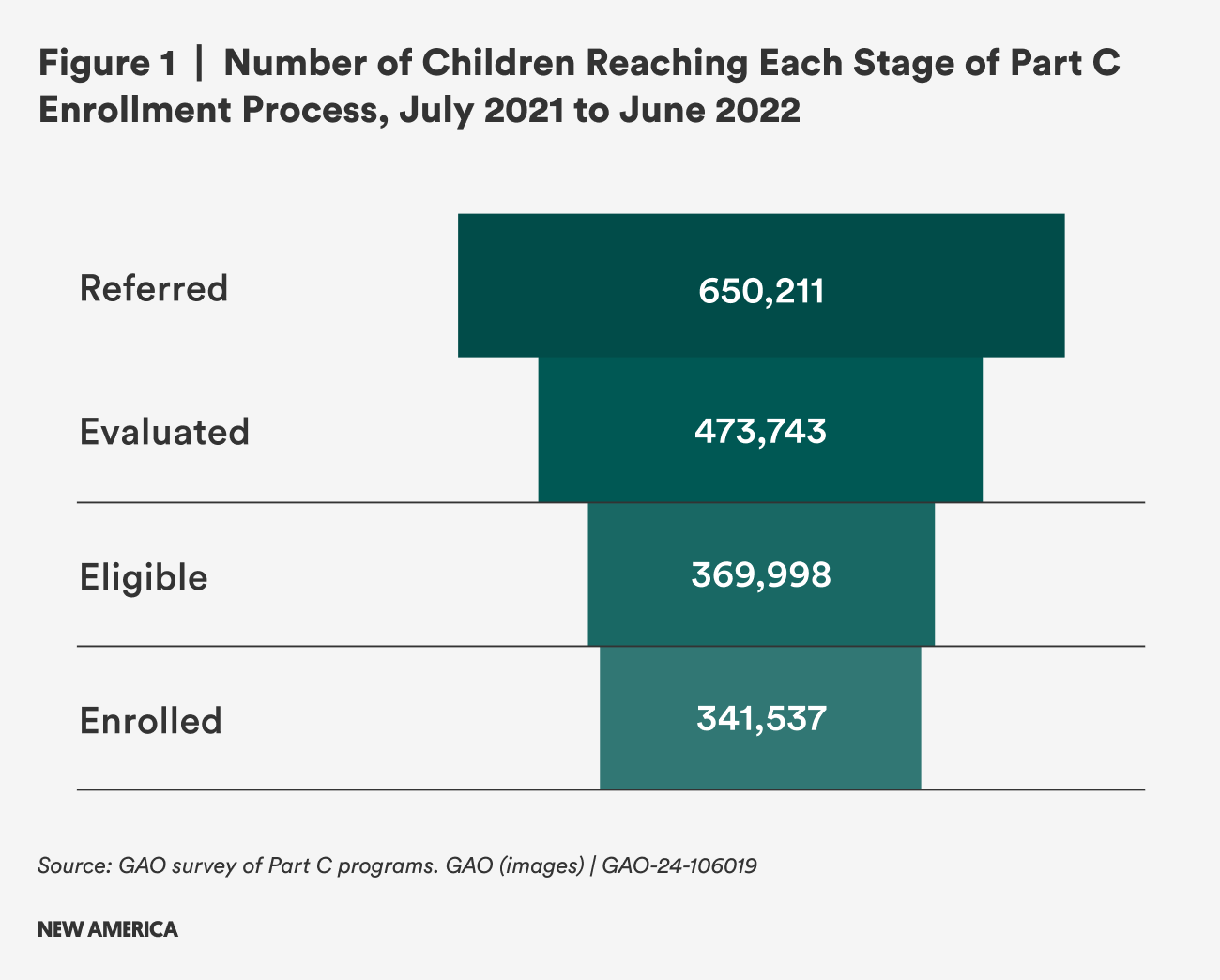
This dropoff may represent a typical program eligibility funnel: After all, not all families who apply for other early childhood or family support programs like Head Start or Medicaid will be approved for services. However, this funnel does not account for another key demographic: children who are likely eligible but never referred. While no national data is available, one study estimated that only 18.7 percent of children in Denver who were likely eligible for early intervention services were ever referred.1
Eligibility criteria for early intervention vary too widely from state to state to estimate the number of children who are likely eligible for services but never identified or referred. According to one study, the percentage of infants and toddlers likely to be eligible ranged by state from 2 to 78 percent, while the proportion of children actually served ranged from 1.48 to 6.96 percent.2 This paints a dispiriting picture and complicates estimation of a nationwide gap.
However, it’s reported that 8.42 percent of U.S. children ages three to seven have been diagnosed with a developmental disability or delay.3 The prevalence among older children is fairly constant, but decreases slightly with age (8 percent among children eight to 12, and 7.8 percent among children 13 to 17). In 2021, there were 11.1 million children under the age of three in the United States.4 Assuming that the prevalence of developmental disability is consistent in the birth-to-three population as it is in three-to-seven year olds, the number of children potentially eligible could be upwards of 934,000 nationwide.
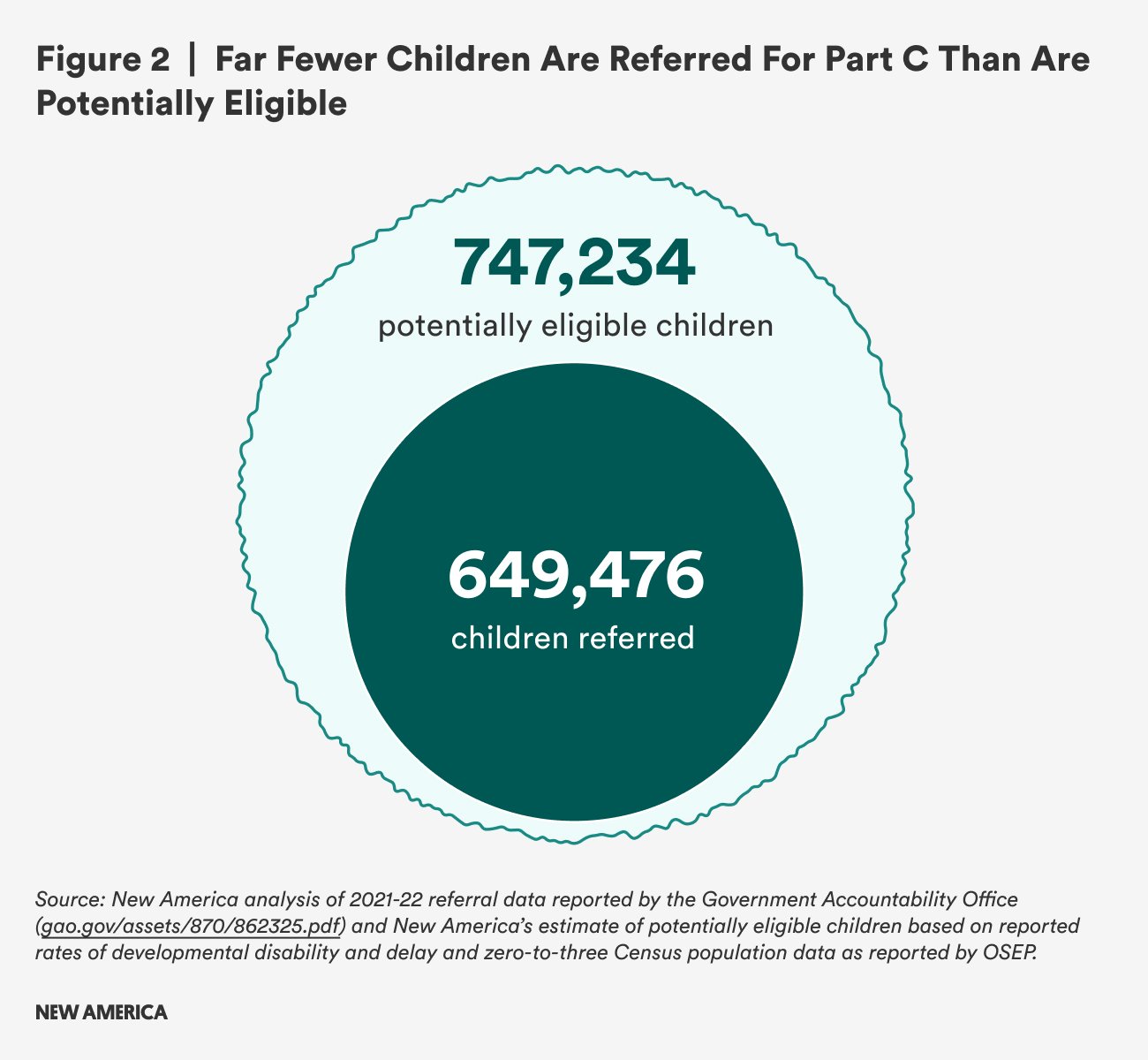
To understand what a gap might look like, we used this general prevalence rate to estimate numbers of children who could potentially benefit from early intervention in states with available referral data. The Government Accountability Office surveyed 56 state and territory Part C programs and found that among the 41 responding locations, just over 650,000 children were referred to early intervention.5 By applying the 8.42 percent prevalence rate to the birth-to-three population in those states, we estimate a gap of nearly 100,000 children who could have been eligible by diagnosed developmental disability (see Figure 2).6 Note that many of these children will not have been diagnosed with a delay or disability yet, which is one of the key challenges of serving children with early intervention services that are by law limited to the birth-to-three age range.
This estimate also undercounts the children who are never diagnosed with developmental disability or delay at all. The Centers for Disease Control and Prevention estimate that one in six children (17 percent) have a disability or delay, diagnosed or not.7 This would make the pool of potential beneficiaries of early intervention services over 1.8 million—if they could be successfully identified and referred in time.
The costs of serving a greater proportion of infants and toddlers would be high, but given the benefits of early intervention to both children and their families, the future and compounding costs of inaction are considerable, if not easily quantifiable.8
One framework to understand the missed opportunity costs is cost avoidance: estimating the extent to which receiving early intervention services may help avoid higher costs in the long run. For example, the Prenatal-to-3 Policy Impact Center summarized an analysis of six states where between 760 and 3,000 children served by early intervention were able to avoid special education services at age 3, with one-year cost avoidance falling between $7.6 and $68.2 million per state.9
However, while cost avoidance and return on investment frameworks help make the case for public programs, the actual experience of families who access (or don’t access) developmental support for their infants and toddlers should be of great interest to policymakers who care about the well-being and even financial security of young children and their parents. If families are denied early intervention, the full out-of-pocket costs for equivalent services could be substantial. Given the developmental benefits to children, the positive impacts on maternal role satisfaction and self confidence, and the poorly understood but very real stressors of caregiving, successful connection to early intervention should be a policy priority for anyone interested in creating conditions where children with disabilities and delays and their families can thrive.
Infants Are Underserved
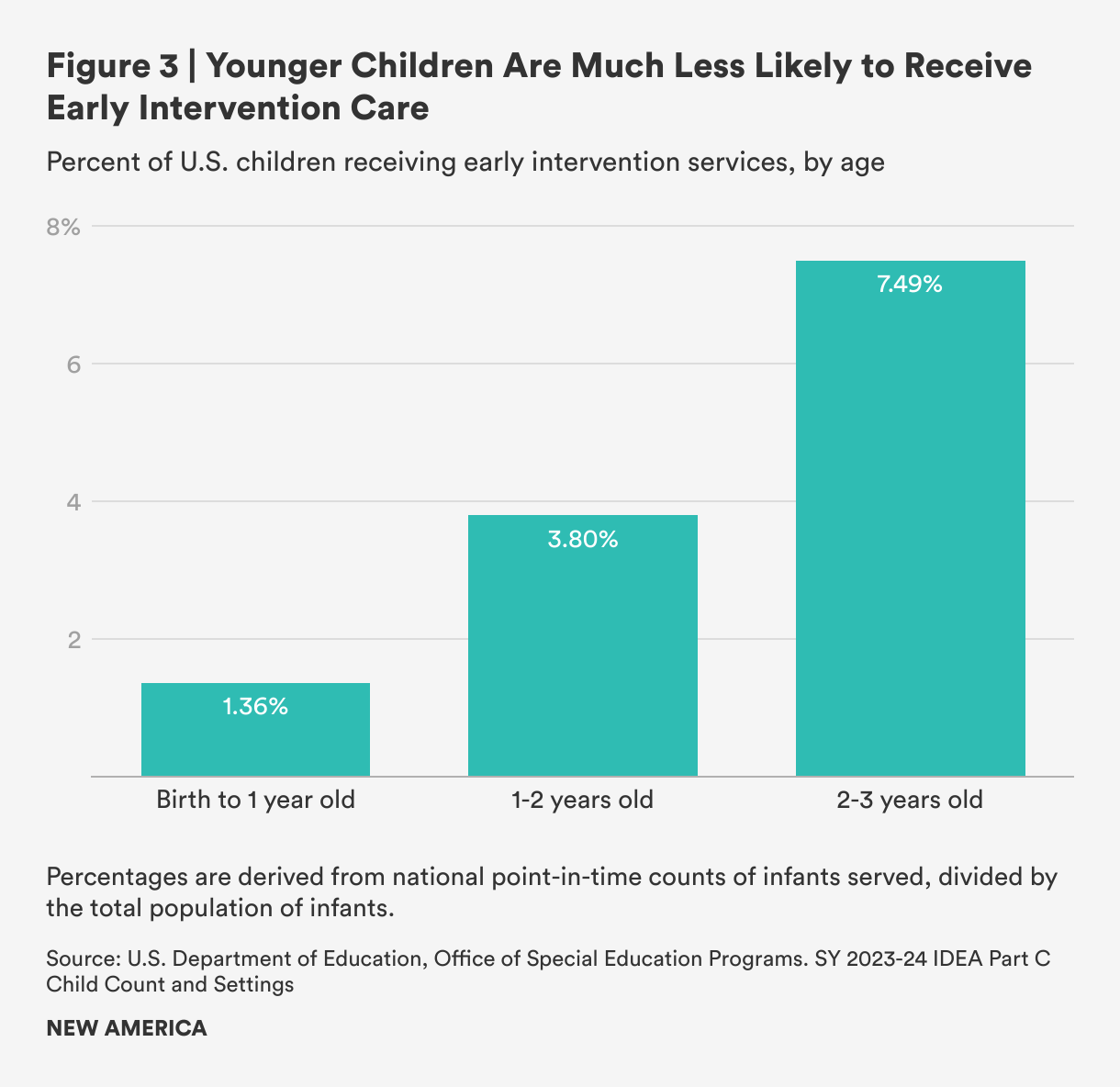
The gap is especially severe amongst infants: Nationally, only about 1 percent of babies under age one received early intervention services compared to approximately 8 percent of children under age three (see Figure 3).10 The service gap to infants can be attributed in part to the limitations of infant assessment: It is difficult to evaluate whether an infant is meeting milestones until they’ve missed them. Some conditions that are identifiable at birth would help qualify more infants for services in the earliest days of their lives, which can help families support their development from the start rather than waiting for delays to appear.
Focusing on early intervention is crucial for babies’ long-term development, so much so that one of the key indicators in state Part C performance plans is the percentage of infants under the age of one receiving an Individualized Family Service Plan. Early identification, referral, and enrollment of younger babies serves a dual purpose: supporting their development at a time of high neuroplasticity, and increasing the dosage of supportive therapies over a relatively short window of opportunity. Toddlers referred and enrolled later may only have a year or even months of benefits before transitioning out of early intervention at age three. Identifying children who might qualify for services while they are still infants is challenging, but states have flexibility in creating policies to make it easier.
Citations
- Beth McManus et al., “Child Characteristics and Early Intervention Referral and Receipt of Services: A Retrospective Cohort Study,” BMC Pediatrics (2020): 20–84, source.
- Steven Rosenberg et al., “Part C Early Intervention for Infants and Toddlers: Percentage Eligible Versus Served,” Pediatrics 113 (2013): 38–46, source.
- Benjamin Zablotsky et al., “Diagnosed Developmental Disabilities in Children Aged 3–17 Years: United States, 2019–2021,” NCHS Data Brief 473 (2023): 1–8, source.
- We used 2021 data to align with the data visualization published by the Government Accountability Office. “IDEA Section 618 Data Products: Static Tables Part C Child Count and Settings Table 4 (2021–2022),” Office of Special Education Programs, source.
- Government Accountability Office, “Special Education: Additional Data Could Help Early Intervention Programs Reach More Eligible Infants and Toddlers,” GAO-24-106019 (2023): 24–25, source.
- The Government Accountability Office conducted a survey of the 56 state and territory Part C programs, and 41 of them provided responses to requests for referral data included in Figure 1. Four of those were U.S. territories: Guam, Northern Mariana Islands, U.S. Virgin Islands, and American Samoa. These territories were excluded from our estimate of potentially eligible children in Figure 2 due to insufficient data, which changed the number of referred children from 650,211 to 649,747. We used the rate of diagnosed disability—8.42 percent among slightly older children—to estimate how many children might have been eligible, but not referred, amongst the zero-to-three population in those remaining states surveyed by GAO. Due to the varying eligibility rates across states, this estimate is illustrative rather than conclusive.
- Mary E. Cogswell et al., “Health Needs and Use of Services Among Children with Developmental Disabilities—United States, 2014–2018,“ Morbidity and Mortality Weekly Report 71 (2022): 453–458, source.
- The legal requirements of Part C present challenges to conducting randomized control trials with non-treatment groups, as all children found eligible for early intervention should be served. As a result, the full costs of not serving children and families has not been quantified or estimated to our knowledge.
- “State Policy Roadmap 2024: Early Intervention Services,” Prenatal-to-Three Policy Impact Center, 2024, source.
- In 2023, 7.7 percent of children under age three received early intervention services when counted cumulatively throughout the year. See: Office of Special Education Programs, “IDEA Section 618 Data Products: Part C Child Count and Settings, Table 10 (SY 2023 to 2024),” U.S. Department of Education, source. Cumulative counts are not available for infants under age one, and this data relies on a “point-in-time” count. Of babies under age one, 1.35 percent received early intervention services and 4.2 percent of children under age three received early intervention services in 2023 according to point-in-time data collected in fall 2023. See: Office of Special Education Programs, “IDEA Section 618 Data Products: Part C Child Count and Settings, Table 4 (SY 2023 to 2024),” U.S. Department of Education, source.
Automatic Eligibility for High-Risk Infants
One way to potentially close the service gap to babies is through policies offering automatic eligibility and enrollment—in other words, focusing attention not just on infants and toddlers already diagnosed with delays and disabilities, but on those at especially high risk of developing them as well. By identifying and connecting these babies and their families to early intervention services based on risk factors rather than diagnosed delay, states can potentially reduce the friction of the typical program enrollment process for families, enabling proactive service delivery and getting eyes on infants’ development instead of waiting for them to struggle.
Current Eligibility Pathways
For the purposes of delivering early intervention services under the Individuals with Disabilities Education Act (IDEA), states independently determine (1) what constitutes an eligible disability or delay, (2) what conditions put infants and toddlers at risk of developing disability or delay, and (3) other high-risk factors.1
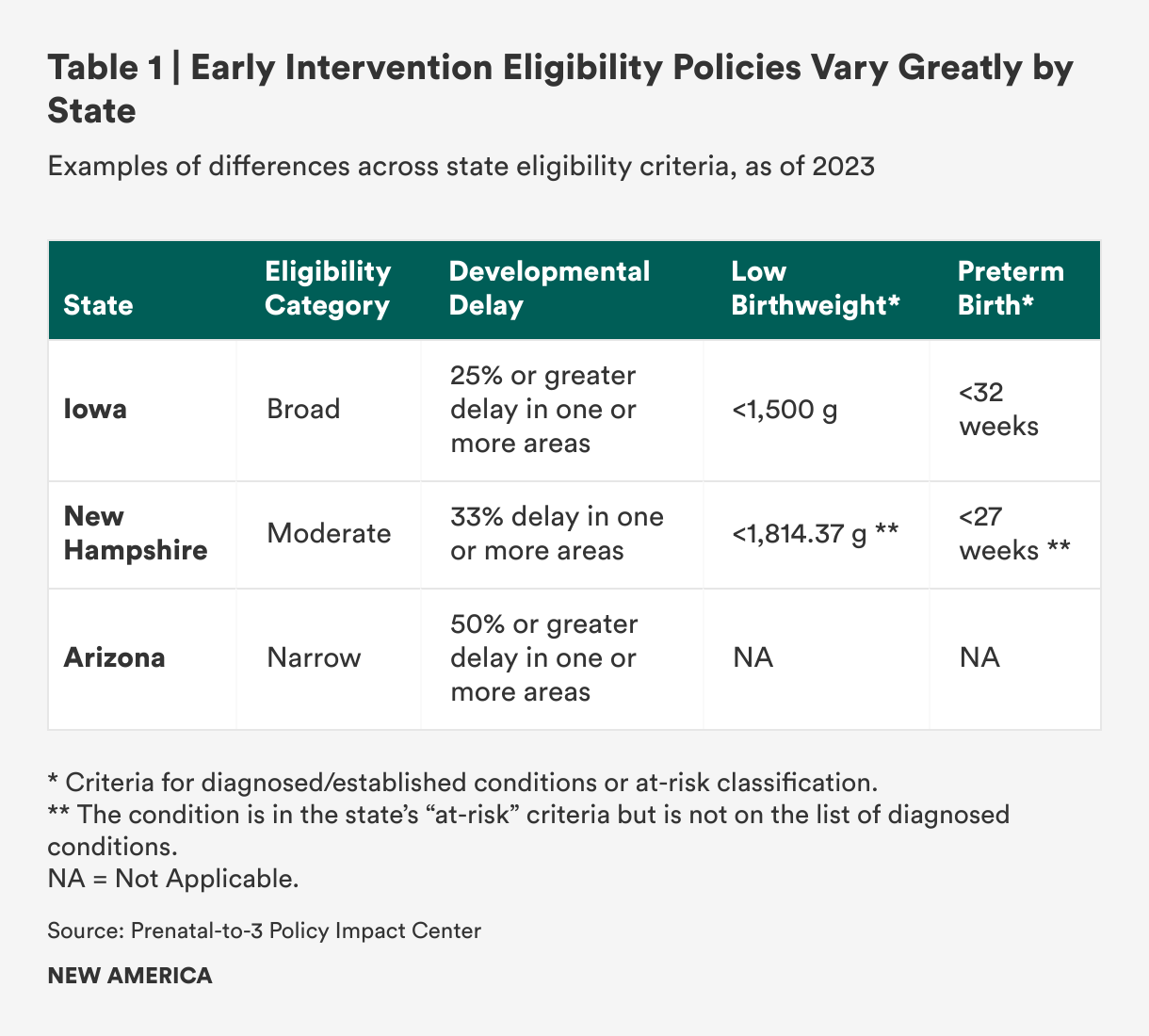
Delays are usually expressed as a percentage to estimate the degree to which a child’s development differs from norms based on chronological age. These metrics vary widely from state to state, both in terms of the percentage of delay required to qualify for services and the number of delays that are present. For example, a child with a 25 percent delay in speech may qualify for services in one state, but not in a state that requires a 33 percent or 50 percent delay (see Table 1). Being diagnosed with any level of delay can be a journey in itself.
For cases where delays are not yet observed but are likely, lists of eligible diagnosed conditions exist. Many are specific conditions like hearing impairment, trisomies, and spina bifida, and these lists can be lengthy and detailed: One study identified over 600 diagnosed conditions across all state lists.2 Some state lists include risk factors covering health and environmental conditions at birth: babies born at low gestational age or very or extremely low birth weight, with neonatal abstinence syndrome or born to a parent with substance use disorder, or who are experiencing homelessness or have child welfare involvement.3 In those states, these conditions—either alone or in conjunction with other conditions—qualify infants as eligible for early intervention.
In general, the need for eligibility policy that is both evidence-based and better aligned across states has been noted by researchers and advocates, but as of now, state variation stands. According to a comprehensive study on states’ eligibility criteria, “despite challenges related to diagnosed conditions, currently states have an OSEP [Office of Special Education Policy]-approved policy regarding their eligibility criteria and are in full compliance with the law, with no requirement for state lists to be based on scientific evidence or otherwise empirically justified.”4
Implementing Automatic Eligibility
Determining eligibility can be time-consuming when it involves waiting for infants and toddlers to miss expected milestones. But, automatic eligibility for early intervention is allowed when a child under the age of three has been diagnosed with a condition that indicates a high probability of delay. Automatic eligibility theoretically allows families of babies with qualifying conditions to bypass complicated determinations and processes, enabling families to start receiving services more quickly. This may be easier to implement for some conditions than others; statistics like very or extremely low birth weight and low gestational age are consistently captured at birth and can be verified through medical records. Importantly, most babies with either or both of those two risk factors are often served in neonatal intensive care units (NICUs) for substantial lengths of time, providing a common touchpoint for connection to services for the babies who may need them.5
Connecting families of low birth weight and preterm babies with early intervention services through the NICU is a promising delivery opportunity. All but 15 states include low birth weight, preterm birth, or both as eligible conditions to qualify for early intervention. Both characteristics are strong predictors of future need for these services, and their prevalence is high in the United States. More than 10 percent of all U.S. babies are born preterm, and most of these infants spend time in NICU. Nearly 9 percent of U.S. babies have a low birth weight, and those with certain health conditions are also likely to be admitted to the NICU. Preterm infants face increased risks of conditions such as cerebral palsy, autism, and attention-deficit hyperactivity disorder.
Connecting families to services through NICU is an established best practice in physical, speech and language, and occupational therapy professions, but also a matter of increasing urgency and potential impact. Medical advancements have resulted in babies born at progressively earlier gestational ages who are able to live and grow. At the same time, high-risk births are all too common as prenatal health care and prevention programs in the United States lag behind many developed countries. The March of Dimes has identified a number of factors that increase the number of preterm infants who are born at risk of developmental delays and disabilities: lack of supportive policies like paid family and medical leave, the prevalence of unhealthy environments, and barriers to primary care to prevent and manage chronic conditions. The growing number of preterm births makes the early identification and enrollment of eligible infants through automatic eligibility even more critical.
Successfully using automatic eligibility to bring early intervention to high-risk infants in the NICU may also help address known disparities in access. Black, American Indian or Alaska Native, and Native Hawaiian or other Pacific Islander mothers are more likely to have preterm and low birthweight infants compared to white mothers, but are also less likely to be served by early intervention services than those of all other races and ethnicities.6 Children from families with lower incomes are 26 percent less likely to receive a developmental screening than children from higher-income families.7 By prioritizing preterm and low birth weight babies, it might be possible to move the needle on these gaps and provide more equitable service to children and families.
Good Policy Does Not Guarantee Successful Implementation
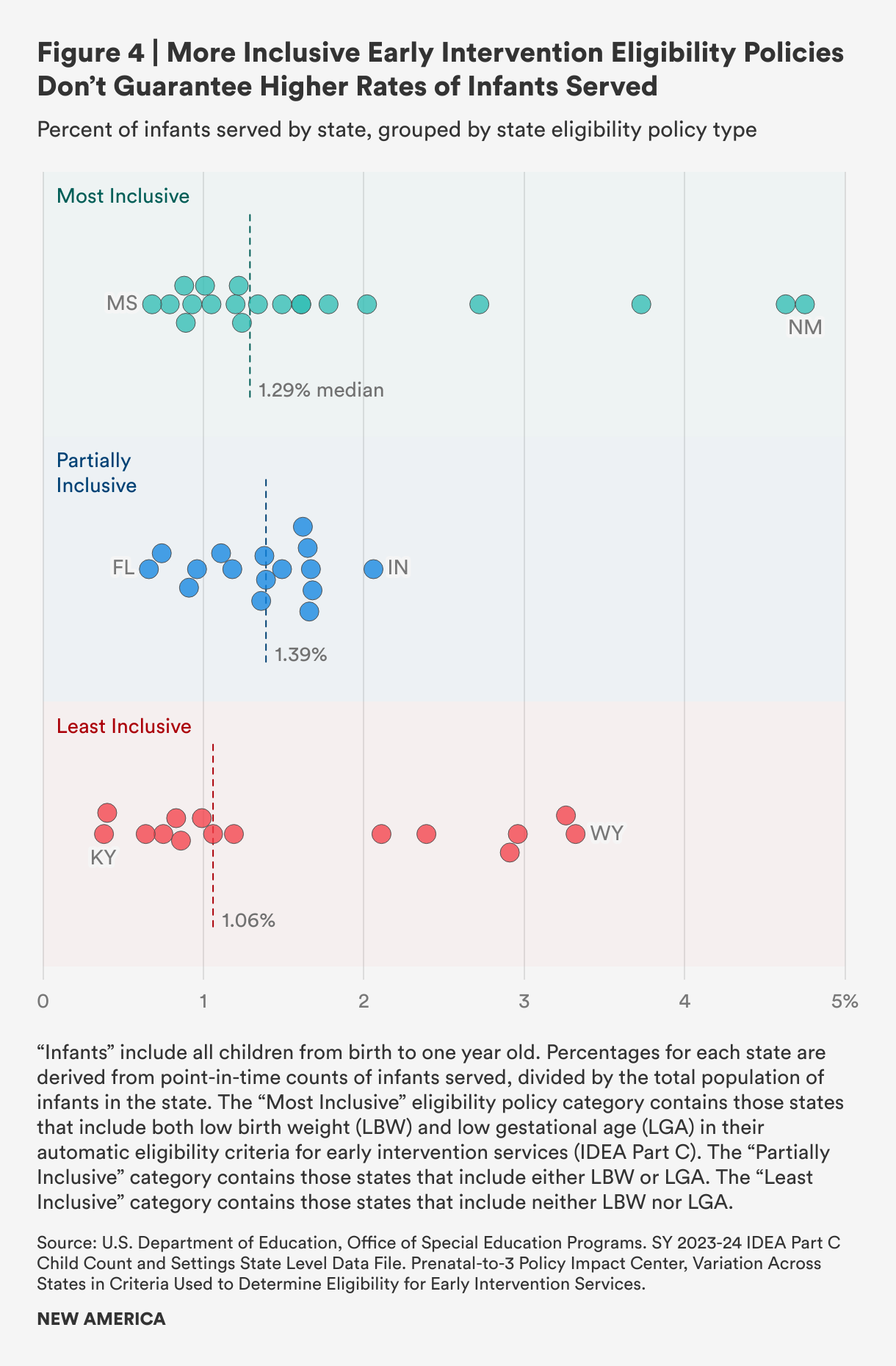
To gauge the potential effectiveness of automatic eligibility, we looked at state eligibility policies’ inclusion of low birth weight and low gestational age and categorized each as “most inclusive,” “partially inclusive,” or “least inclusive” across all 50 states and the District of Columbia.8 We looked for any correlation between inclusivity and the percentage of infants served according to program data (see Figure 4). We found that policies characterized as most inclusive did not necessarily correspond with a higher rate of infants served, while some states with least inclusive eligibility policies serve a relatively high percentage of infants. Our analysis shows that strong policies alone do not necessarily result in higher early intervention service rates for infants and their families, and we theorize that implementation challenges are likely a factor, along with longstanding underfunding.
Given the complexity of eligibility policies, our analysis is illustrative but not conclusive in drawing a line between eligibility policy for low birth weight and premature babies and service to infants. Future studies should further analyze the variability of eligibility criteria and their association with early intervention services rates, along with other variables such as funding. If serving more infants in early intervention is a goal, state leaders could use better information about where policies are working well to bring more infants into the system, and how these policies could be better implemented.
The factors influencing low rates of service to infants are complex, but whatever the reasons, the disconnect has implications for children and families who should qualify. A recent article in the Hechinger Report highlighted a case in Illinois where children who were eligible by state criteria were not connected with early intervention services.9 As a result, these children missed out on services that are designed to encourage their healthy development and long-term success that they are entitled to receive. This is not isolated: A 2017 study in an Oregon hospital found that 71.5 percent of low birth weight infants were not enrolled in early intervention services by their first high-risk infant follow-up appointment, and of those not enrolled, 42.1 percent would qualify for services due to high-risk conditions.10
While it is unclear how widespread the disconnect between automatic enrollment and service delivery is, either in Illinois or across the country, it represents an all-too-common problem: a strong policy to help families with young children that may not meet their needs because of flawed implementation.
Citations
- IDEA part C regulations include five categories of delay—physical, cognitive, communication, social or emotional, and adaptive—along with a non-exhaustive list of potentially eligible conditions: chromosomal abnormalities; genetic or congenital disorders; sensory impairments; inborn errors of metabolism; disorders reflecting disturbance of the development of the nervous system; congenital infections; severe attachment disorders; and disorders secondary to exposure to toxic substances, including fetal alcohol syndrome. See: “§ 303.21 Infant or Toddler with a Disability,” Code of Federal Regulations (2025), source.
- Brian Barger et al., “State Variability in Diagnosed Conditions for IDEA Part C Eligibility,” Infants and Young Children 32 (2019): 231–244, source.
- For simplicity throughout this report, we will use “low birth weight” for both very low (>1500 grams) and extremely low (>1000 grams) birth weight, and use “preterm” in lieu of “low gestational age,” typically defined as any birth before 37 weeks.
- Barger et al., “State Variability in Diagnosed Conditions for IDEA Part C Eligibility,” source.
- While national data is not readily available, one study found that 56.3 percent of preterm infants were low birthweight, and 72.4 percent of low birthweight infants were preterm, demonstrating some of the potential overlap between these two conditions. See: Stephanie A Leonard et al., “Associations Between Preterm Birth, Low Birthweight, and Postpartum Health in a Predominantly Hispanic WIC Population,” Nutrition Education and Behavior 46 (2014): 499–505, source.
- Latoya Hill et al., Racial Disparities in Maternal and Infant Health: Current Status and Efforts to Address Them (Kaiser Family Foundation, 2024), source; Office for Civil Rights, 45th Annual Report to Congress on the Implementation of the Individuals with Disabilities Education Act (Department of Education, 2023), source.
- LaRue Allen and Rebekah Hutton, eds., “Opportunity Gaps in Early Care and Education Experienced by Children from Birth to Pre-K,” in Closing the Opportunity Gap for Young Children (National Academies Press, 2023), source.
- “Variation Across States in Criteria Used to Determine Eligibility for Early Intervention Services,” Prenatal-to-3 Policy Impact Center, Vanderbilt University, source.
- Sarah Carr, “Parents of Premature Babies Struggle to Get Help Their Children Are Entitled To,” Hechinger Report, January 23, 2025, source.
- Kristi Atkins et al., “Part C Early Intervention Enrollment in Low Birth Weight Infants At-Risk for Developmental Delays,” Maternal and Child Health 21 (2017): 290–296, source.
Stakeholder Perspectives on Service Gaps
Family Perspective
For this initial discovery sprint research, we did not set out to engage directly with families for their perspectives on transitions of preterm and low birth weight infants from the neonatal intensive care unit (NICU) to home. For more extensive engagement in the future, trauma-informed protocols would be used to include family perspectives.
That said, the team did incidentally hear from families with personal NICU experience, as some of the subject-matter experts we spoke with have children who were low birth weight or preterm babies. These conversations reinforced findings from literature, online parenting groups, and others working in the field: Stays in the NICU are frequently lengthy and often traumatic. At the very least, they are an overwhelming moment in a family’s life.
What we learned:
- Birth can feel like an impractical time to enroll families in services. The Federal “Birth of a Child” Life Experience team created a Zero to 5 Journey Map tracing the steps of low-income mothers from pregnancy through early childhood, including various touchpoints where connection with supportive services might work well. The document points to a “birth-time haze” as a barrier to enrolling families in supportive programs. As their report states: “Birth is an overwhelming and impractical time to learn about and apply for benefits. Facts are easily forgotten and physical information is often misplaced.” This is critical to remember when planning service connections around childbirth and hospital discharge. Reducing the burden associated with applying for and enrolling in supportive programs could make birth a more practical time to connect families.
- Mental health challenges specific to NICU stays amplify the typical challenges of birth. The hospitalization of newborn infants compounds the typical stress and exhaustion many new parents experience. We heard from NICU practitioners that parents are wrestling with extremely difficult questions: “Will my child survive? Will they be ‘broken?’ How long will we be in this stressful, strange environment?” Additionally, families may face financial stress due to missed work, hospital bills, or both. It should not be surprising that 35 percent of mothers and 23 percent of fathers experience acute stress disorder in the days after hospital stays, with 15 percent and 8 percent experiencing ongoing stress disorders, respectively.1
It is within this soup of exhaustion and emotion that parents must make decisions about next steps for their infant transitioning out of NICU care. Conversations and decisions about early intervention cannot and should not be avoided, even though the environment and timing are, as noted above, a challenge. Some aspects of the NICU birth experience, notably the length of stays and exposure to supportive therapies for infants, in fact make it an optimal time to expose, educate, and even enroll families in supportive services prior to discharge, including early intervention.
Many parents are not aware that early intervention is an important program available to them in the suite of early care and education services for young children. For parents who are not notified about automatic eligibility or enrollment in early intervention services, these children may be locked out of services unless a delay is noticed and their child is referred for evaluation based on the observation of a future clinician.
Parents who are informed about eligibility for services may still opt not to evaluate or enroll for a number of reasons:2
- Enrollment in early intervention can be confusing. The referral and enrollment process is different and more logistically complex than other programs that parents apply to directly, like Medicaid or the Supplemental Nutrition Assistance Program.
- There are many misconceptions and feelings of mistrust about early intervention services. Misconceptions occur when families believe that they are not eligible or that services are not compatible with their other care. For example, they may not realize that they can receive early intervention alongside home health services for medical needs, or home visiting for postpartum support (such as through the Maternal, Infant, and Early Childhood Home Visiting Program). Mistrust is a result of fears that interacting with services may trigger unintended consequences. Families may mistrust social workers and see home-based early intervention services as surveillance, or fear attracting the attention of the child welfare system by applying for public services.3
- Both pediatricians and families of infants with NICU stays sometimes opt for a “watch and wait” strategy. Families of infants with NICU stays have been through a lot, and some very low birth weight and low gestational age babies do not experience delays at all. According to a study on barriers to evaluation, some parents may choose to step back from services for a time, and initiate them later if possible delays are observed. They may also prefer to work with their child on their own before seeking early intervention.4 On the other hand, some families would prefer closer monitoring and expert assessment of their infants’ development, but are dissuaded by pediatricians who prefer to wait for signs of delay to appear, as one study focusing on rural infants and toddlers found.5
- Coordination of therapies can be complex and burdensome. It can feel like another job to coordinate regular therapies. The United States lags far behind other countries in access to paid family and medical leave programs that would help people attend to their prenatal health, potentially avoiding unsafe births to begin with, and to care for their children after birth or adoption. These insufficient leave policies (with a few important exceptions) become even more pronounced when families are contending with a complicated birth and long NICU stay. Some parents have to go back to work and do not have the bandwidth to manage what feels like “one more thing.” Even if they are not working, they might prioritize quiet time to bond as a family, caregiving for other family members, or other responsibilities.
- Social and economic factors like income impact family participation. Not all families will opt into early intervention when offered, and not all families are equally equipped to take advantage of the services. For example, one study found that for every $10,000 decrease in median family income, the odds of accessing adequate early intervention services decreased by 24 percent.6 Another study of early intervention access after NICU discharge in a Medicaid population identified multiple barriers for these families in particular: scheduling visits is challenging, transportation may be an issue when home services are not available, or they fear that early intervention services will incur out-of-pocket costs that they can’t afford.7 Mental and behavioral health issues like substance abuse disorder can also be a factor.
Provider Perspective
We interviewed key members of NICU teams to complement what we learned from the literature. The providers we spoke to were enthusiastic about the importance of connecting families of automatically eligible infants in NICU with early intervention services, and pointed both to good practices and challenges in making those connections.
- NICU stays can be difficult and lengthy, but they present an opportunity to build trust with families of automatically eligible infants. Many families experience a lot of waiting and other “downtime” during NICU stays that can be—and often is—leveraged to educate them about neonatal care and connect them to helpful resources like early intervention. This can be particularly powerful when families have developed good communication and high trust with staff.
- However, family availability to spend time with their preterm or low birth weight babies in NICU varies. The time families can commit to NICU visits will vary depending on transportation, distance from home, and work and family obligations.8 The availability of leave programs (paid or not) and job protection may also affect families’ ability to be bedside.9 Some families may go back to work immediately to bank their paid or unpaid leave or paychecks for when babies come home. One NICU staff member noted that some parents find work to be a welcome respite from the hospital environment. Another noted an influx of parents at the end of the work day arriving to spend time with their babies.
- Family exposure to early intervention during this time is critical. Preterm and low birthweight babies in NICU will begin receiving services to encourage their healthy growth and development as quickly as possible, and engaging families will help them support infant development at home. This engagement may not come directly from therapists, depending on schedules. Many NICU staff—particularly bedside nurses—are critical partners in transitioning caregiving back to the parents during the hospital stay. They can use that time to educate families about ongoing support for healthy development, including early intervention services.
- Consistent discharge procedures are a must. Interdisciplinary guidelines for NICU transition planning recommend assessing every family for early intervention services eligibility and then referring eligible families prior to discharge.10 While discharge procedures might be informed by widespread guidance, they can vary from place to place, and even well-designed discharge procedures have limitations. Procedures need to work for shifts across nights, weekends, holidays, and staffing changes. Medical social workers can provide excellent support to families as they prepare for discharge, including written material to support parent education and direct referrals to early intervention services. However, they do not work around the clock, so discharge procedures should be clear and transferable across disciplines.
- Even the most consistent procedures will still not work for everyone. Automatic referral and well-established discharge processes are important. But even with strong procedures in place, staff might miss opportunities to make referrals at discharge, and families might not have the wherewithal to act on them. In one study, 14 to 28 percent of automatically eligible babies who returned to the NICU for developmental clinic visits at four months still needed early intervention referral, even when they’d been seen by primary care physicians, signaling a missing touch point in pediatric care.11
- Providers struggle to connect with all families, but service gaps are bigger for certain groups. Even though the health, social, and education systems involved in supporting these infants are highly interconnected, they lack coordination and cause frustrating administrative hurdles for families. Black families, families with low incomes, and non-English-speaking families have lower access to early intervention and high-risk infant follow-up programs following NICU stays.12
- Pediatricians are critical partners who may not be well integrated into automatic referral through eligible conditions. We did not conduct a 50-state scan of eligible condition lists, but the lists we did review were not always easy to find or written in plain language. Given the complexity of early intervention eligibility policy, it is unsurprising that pediatricians tend to rank their understanding of diagnostic criteria for early intervention lower than early intervention staff.13
- Better guidance for pediatricians on eligibility criteria and infant and family benefits of early intervention may help. Many pediatricians are enthusiastic partners in referral to early intervention, but sometimes they hesitate to refer. Lack of guidance on early intervention referral procedures likely contributes to pediatricians’ hesitation in referring families and reliance on a “watch and wait” approach.14 Pediatricians may delay referring when a child has delays in only one developmental domain rather than multiple, or when parents are hesitant about referral. Better guidance on the benefits of automatic referral for eligible infants—for both infants and their families—might help move the needle.
- Pediatricians and hospital staff may hesitate to refer families to early intervention when there are wait lists or delays getting services. Pediatricians and hospital staff with knowledge of program scarcity may not be willing to refer families to services they will have difficulty accessing because of provider shortages or long wait times.
Administrator Perspective
- There’s “no wrong door” for referring families, but the doors need to be more accessible. States offer many different ways to refer children to early intervention state agencies, including phone, fax, email, and websites. Administrators note that this variety of avenues creates a “no wrong door” approach to increase referrals. However, barriers at these referral points can inhibit connections. A survey of state early intervention agency Part C coordinators found that nearly three-quarters (72 percent) of state referral forms were only available in English. Families accounted for 30 percent of those making the referrals, and six states reported families as the most common referral source, making the availability of forms in multiple commonly spoken languages a priority to reach wider networks. Most state referral forms (81 percent) were available as electronic documents and required downloading plus handwritten signatures. Most of these methods require several steps across multiple agencies, which increases the odds of human error (such as omitting information) that may slow down the process.15
- Good communication and interagency collaboration are important for successfully connecting families to early intervention. Information about children with delays and disabilities, as well as their families, is not well integrated between health and education data systems, which exchange little or no information. For example, there is a wide variation in the functionality and capabilities of early intervention referral forms.16 While electronic health record systems might note referral to early intervention services and other helpful follow-up appointments, many early intervention coordinators and agencies do not have access to those systems, and the referrals themselves don’t confer records access. This requires early intervention agencies to make separate records requests to hospitals and pediatrician offices when needed, slowing down the referral and evaluation process.17
- Referral requirements are confusing. Many pediatricians and early intervention staff report that they need more guidance as they are not clear on how to refer, what information to include, who is responsible for getting parental consent, and how to use state lists of approved conditions to determine whether to refer.18 This confusion leads to missing information, missed opportunities for referrals, and slower timelines from referral to enrollment.
- There is lack of clarity regarding services provided through a medical model versus services focused on education and social support like early intervention. Many preterm or low birth weight babies will need continued medical attention, and some may even need home or respite care. There is genuine confusion over who is best equipped to provide intervention services to very preterm babies. According to some of the experts we spoke with, serving this population may require specialized skills, and there may not be enough early intervention providers with sufficient experience providing this level of care. However, supporting parents and caregivers is also an important focus of early intervention. Early intervention or other supportive services, such as home visits, could be effective at supporting the emotional and mental health needs of parents while skilled nurses support the physical health and development of their babies. The choice between a medical or family-centered model is an unresolved source of tension among dedicated people who all want good things for NICU graduates and their families, even when they are clear-eyed about the advantages and disadvantages of multiple approaches.
Citations
- Debra Lefkowitz, Chiara Baxt, and Jacquelyn Evans, “Prevalence and Correlates of Posttraumatic Stress and Postpartum Depression in Parents of Infants in the Neonatal Intensive Care Unit,” Clinical Psychology in Medical Centers 17 (2010): 230–7, source.
- Manuel Jimenez et al., “Barriers to Evaluation for Early Intervention Services: Parent and Early Intervention Employee Perspectives,” Academic Pediatrics 12, no. 6 (2012): 551–7, source.
- Jimenez et al., “Barriers to Evaluation for Early Intervention Services,” source.
- Jimenez et al., “Barriers to Evaluation for Early Intervention Services,” source.
- Kalli Decker et al., “The Early Intervention Referral Process for Rural Infants and Toddlers with Delays or Disabilities: A Family Perspective,” Maternal and Child Health 25 (2021): 715–723, source.
- Marie Fefferman, Bree Andrews, and Michael Msall, “Disparities in Access to Early Intervention Services for Extremely Preterm Infants by Family Income,” International Public Health 9 (2017): 155, source.
- Ashwini Lakshmanan et al., “Connecting to Early Intervention Services After Neonatal Intensive Care Unit Discharge in a Medicaid Sample,” Academic Pediatrics 22 (2022): 253–262, source.
- Stephanie Bourque et al., “The Association of Social Factors and Time Spent in the NICU for Mothers of Very Preterm Infants,” Hospital Pediatrics 11 (2021): 988–996, source.
- Ashley Weber et al., “Paid Family Leave to Enhance the Health Outcomes of Preterm Infants,” Policy, Politics, and Nursing Practice 19 (2018): 11–28, source.
- Vincent Smith, Kristin Love, and Erika Goyer, “NICU Discharge Preparation and Transition Planning: Guidelines and Recommendations,” Perinatology 42 (2022): 7–21, source.
- Michelle Greene and Kousiki Patra, “Part C Early Intervention Utilization in Preterm Infants: Opportunity for Referral from a NICU Follow-Up Clinic,” Research in Developmental Disabilities 53–54 (2016): 287–295, source.
- Litt et al., “Ensuring Optimal Outcomes for Preterm Infants After NICU Discharge,” 146, source.
- Asha Yadav, Randall Alan Phelps, and Jane Squires, “Knowledge of Established Conditions List and Associated Policies and Procedures Among Pediatricians and Early Intervention Personnel,” Developmental & Behavioral Pediatrics 46 (2025): e64–e70, source.
- Asha Yadav, “Part C Early Intervention Referral and Eligibility for Children with Diagnosed Medical Conditions: An Exploratory Study in Two States,” presented to the Department of Special Education and Clinical Sciences and the Division of Graduate Studies of the University of Oregon in partial fulfillment of the requirements for the degree of Doctor of Philosophy (2023), 91, source.
- Benjamin Sanders et al., “Early Intervention Referral Information, Transmission, and Sources—A Survey of State Part C Coordinators and Analysis of Referral Forms,” Developmental & Behavioral Pediatrics 43 (2022): e153–e161, source.
- Sanders et al., “Early Intervention Referral Information, Transmission, and Sources,” source.
- Yadav, “Part C Early Intervention Referral and Eligibility for Children with Diagnosed Medical Conditions,” 66, source.
- Yadav, “Part C Early Intervention Referral and Eligibility for Children with Diagnosed Medical Conditions,” source.
Promising Practices
The underenrollment of infants in early intervention is not a new or understudied problem. The experts we interviewed were aware of gaps in service, and literature confirmed the gap’s persistence over time despite the deficiencies being acknowledged. A 2016 study used qualitative research with families and providers in two states to better understand barriers to the delivery of early intervention to preterm infants.1 The authors categorized four types of gaps to produce a strong resource offering 22 recommendations for innovation in early intervention systems using a Chronic Care Model framework organized by framework component, estimated timeframe for implementation, and responsible stakeholder. Nearly a decade later, the gaps still exist, as do widespread opportunities to implement these recommendations.
Using expert interviews and recent research, we present an updated list organized by type of fix: procedural, cultural, technical, and structural.
Procedural Fixes
A major challenge to smoothing enrollment of infants from neonatal intensive care unit (NICU) into early intervention services is the wide variation between policies and procedures from state to state, county to county, and hospital to hospital. While care protocols like high-risk infant follow-up have been widely adopted, the practice itself can be hard to access.2 Despite efforts to tackle this, programs can still be underenrolled.3 But even amid the challenges of connecting families to services like high-risk infant follow-up and early intervention, there are promising practices to improve referrals and participation.
- Leverage the “captive audience” nature of NICU, especially through bedside nursing. One study identified patient education strategies as one of the most effective tools for encouraging attendance at follow-up appointments in the developmental clinic: In an anonymous survey of parents who attended the first visit, 95 percent indicated bedside education was the most important factor in clinic attendance.4 Most infants receive therapy while in the NICU, primarily speech therapy to help them learn to feed, but occupational and physical therapists may also provide services. These care team members can also help prepare parents for continuation of services through early intervention.
- Families appreciate a warm hand off to services. In order to help families feel comfortable in the transition from the hospital to community-based early intervention services, NICU staff should provide the family with a warm hand off that includes a personal connection. Early intervention providers can visit NICUs in person if possible by attending developmental clinics, or they can attend multidisciplinary or discharge meetings remotely if needed.5 In Project Initiate, hospital staff scheduled a virtual orientation meeting between families and early intervention prior to discharge. These warm hand offs helped “establish early rapport, clarify expectations, and contributed to more timely initiation of services after discharge.”6
- Be open to adopting new models for connection and service. A recent Start Early report updating some of the work first shared through Project Initiate summarizes a model where early intervention coordinators are colocated with NICUs, allowing families to go home with not just a referral but an Individualized Family Services Plan (IFSP) in hand, having initiated services during their stay. The model also includes closer hospital–early intervention coordination for information sharing, including with local early intervention coordination offices to facilitate continuity of services once infants go home.
- Integrate early intervention into discharge planning. A 2021 study of Medicaid users flagged integration of early intervention into discharge planning as a helpful practice, and a 2022 study affirmed it: “Assess every family for Part C of Individuals with Disabilities Education Act (IDEA) eligibility and make a referral to qualifying families prior to discharge.”7 Making early intervention referrals far in advance of discharge may start the clock too early on a 45-day timeline to service; this may be unhelpful to early intervention coordinators. Regardless, making sure early intervention is incorporated into a standard discharge checklist helps ensure that the connection is made, no matter who is managing the process on weekends and holidays.
- Family navigation and advocacy from care providers may be helpful. One NICU provider suggested that peer support from families who have already navigated early intervention services might be helpful for hesitant families. Peer navigation has shown promise in other perinatal and maternal health contexts, and one study found that providing peer navigation to families resulted in a 10 percent increase in early intervention participation.8 In a different study, families noted that they sometimes got better service from early intervention offices when a hospitalist called on their behalf than when they called directly.9 A “medical–legal” partnership connecting patients and families with legal support in medical settings helped families work through checklists and “unstick” the process.10
- Make lists of eligible conditions easy to understand and find. A 2020 study of state lists of qualifying conditions noted that “the wide heterogeneity in the number and type of diagnostic conditions listed across states” could contribute to imbalances in which children can access early intervention services. Providing ready access to lists of conditions is a simple step to facilitate access.11
- Incorporate early intervention eligibility criteria into a tool or flowchart for providers to easily determine whether and how children qualify for services. This recommendation is one of the 22 recommendations identified in the 2016 paper cited above.12 The chart needn’t be paper, nor does it need to be restricted to early intervention, as there are many supportive programs that can benefit NICU families. Such screeners exist for early care and education, like South Carolina’s First 5 SC, and for tax credits and public benefits programs, like MyFriendBen.
- Create universal referral platforms. Training on referral and eligibility determination processes can help pediatricians and early intervention staff more efficiently refer and collaborate. A statewide, web-based referral form (like Michigan’s) for pediatricians, families, and other referrers can list centralized contact information alongside referral policies and protocols to minimize confusion about how to refer and what information to include. Including parental consent information compliant with HIPAA (the Health Insurance Portability and Accountability Act) and FERPA (the Family Educational Rights and Privacy Act) can expedite referral processes and avoid confusion about who is responsible for obtaining consent.
- NICU providers should share referrals with primary care physicians. One NICU set a goal to improve attendance at their high-risk developmental clinic from 60 to 80 percent, and one of the methods they used was formatting a standard referral letter to infants’ primary care physicians.13 This relatively low-lift task helped smooth the transition of care from NICU to pediatrician and could be adopted for early intervention referrals as well. This step could also help pediatricians whose self-reported understanding of qualifying conditions is lower than early intervention staff.14
- Written materials are still useful “takeaways” for family learning. Educational materials staff give to families at discharge should be available in various languages and accessible in paper and digital form.15 Importantly, materials should make it clear that parents can self-refer to early intervention if they are concerned about their infant’s development.
- Adopting a multipronged approach may be necessary. Gaps in early intervention services to preterm babies and other infants in the NICU with other eligible conditions or diagnoses are not driven by one particular thing, nor will there be a magic bullet solution. One program tackled gaps in neurodevelopmental services to NICU graduates by focusing on three drivers of success in improving uptake: consistent communication, standardized processes, and family integration.16
Programs created to support families discharged from the NICU also show promise for increasing early intervention connections:
- The Baby Bridge program in St. Louis (also known as NICU Transition Services at Washington University Occupational Therapy) provides continuity of care between discharge and connection to community-based therapy services like early intervention. A Baby Bridge therapist builds a relationship with parents while in the NICU that continues after discharge. Its pilot study showed that the program connected more families, more quickly, to early therapy services such as early intervention.17
- The Hospital-to-Home program in the Seattle area creates a focus area within the state early intervention program specifically for families exiting the NICU. Babies are often evaluated for early intervention and enrolled two weeks after NICU discharge. Specialists in the program, including family resource coordinators and physical, speech, and occupational therapists, receive training in working with preterm infants and in perinatal mood disorders. The program’s systems change team, funded privately and publicly, provides three-day training to early interventionists across the state in order to replicate the model, since many therapists do not have backgrounds working with preterm babies.
- Arizona’s Smooth Way Home program aims to strengthen transitions from the NICU to home in part by increasing early intervention connection prior to or just after NICU discharge. A statewide community taskforce with members from state agencies, early intervention services, parent advocacy groups, and NICU staff inform the program.
- Some states like Washington have early intervention connection programs specifically to address neonatal abstinence syndrome among infants and substance use disorder among adults. (Neonatal abstinence syndrome impacts infants directly, while parental substance use disorder is a high-risk condition for infants.)
- Nebraska has been working on this area since 2000. They provide funding for a program called Developmental TIPS (Tracking Infant Progress Statewide). This program ensures developmental screening (with parental consent) for infants who were in the NICU for at least 72 hours. There is criteria for direct referrals to early intervention; otherwise, the infants go through periodic screening and are then referred as needed.
Cultural Fixes
Some barriers to early intervention enrollment are cultural in nature, and solutions may be driven by focusing on staff training, patient education, and culturally competent care.
- Families need responsive, human-centered assistance navigating decisions about early intervention. Many families exiting NICU are eager to initiate early intervention, but others hesitate. When family hesitation is due to a preference, those preferences can be respected while relationships with providers are kept warm or personally engaged. Parenting is a nonstop series of decisions, some of them easier than others. To support their choices, families need high-quality information in both print and electronic formats that is written in plain language (and in languages other than English). They may also need easy on-ramps to services should they later decide to opt in. When their hesitation stems from specific constraints, those constraints should be mitigated with available wraparound supports such as transportation assistance and interpretation when possible. While connection to early intervention services can be initiated in NICU for automatically eligible babies, these stays should not be the final touchpoint for families who are hesitant, or who could use more support connecting with services.
- Bridge language and cultural barriers with families. More multilingual NICU and early intervention staff would improve communication between families and providers who often rely on limited interpretation services and technology such as iPads.
- Reassure families that early intervention services are support, not surveillance. Literature and interviewees alike pointed out families’ worries that early intervention is synonymous with child protective or immigration services. Hesitant families might benefit from a connection with families within their own communities who can explain what to expect from early intervention. They could also meet early intervention staff in person or remotely in advance of enrollment.
- Strengthen wraparound services for hard-to-reach families. NICU discharge guidelines published in the Journal of Perinatology recommend direct referral to early intervention and a comprehensive home and family need assessment to understand the family’s readiness to assume full-time care for a medically complex infant.18 This assessment can include the family’s transportation options, access to food, and financial stability. Early intervention is just one of many benefit programs that low-income families may be eligible for that will support the development of their child.
- Benefit screeners may help guide the process of connecting families with supports, and providers can get creative. Some states have adopted eligibility screeners that will help families understand what is available to them or assist a social worker who is walking them through options. In other states, understanding eligibility will be a more fragmented experience, and hospital staff create physical binders of reference materials for families. In either case, access to major state and federal programs can be augmented with information about other supports such as food pantries, clothing swaps, and other local resources. One health provider we spoke with hosted a baby closet of supplies themselves.
- Try to meet families where they are. Families of NICU babies are not a monolith. Depending on their work schedules, overall family needs, physical and mental health, home environment, and access to transportation, some families prefer to receive services at home, some will prefer to go to a clinical environment, and others will prefer telehealth. While the latter may not be the ideal mode of delivery, it is better than a family refusing services because the delivery model doesn’t work for them.
- Close the gap between medical models of follow-up care and family-centered early intervention services. Transition program staff cited the need to increase buy-in from some NICU staff into the benefits of early intervention. Developmental clinics mandated by Level III and IV NICU are valuable assets in infant follow-up care, but they may focus more on medical aspects of infant development and are not a substitute for ongoing therapeutic support. Staff noted that focusing on early intervention’s emphasis on perinatal mental health and family-based social and emotional support helps create hospital interest, since those are services that are not always provided by hospital specialists. One study noted that “high-risk infant follow-up, like most post-discharge health services, has some shortcomings, including: unclear goals; inadequate support for infants, parents, and families; fragmented service provisions; poor coordination among providers; and an artificially foreshortened time horizon.”19 This suggests the need for a new model for assessment of goals and outcomes based on touchpoints rather than medicalized approaches. This aligns with other efforts to map services to specific family experiences.
Technology Fixes
States have employed a variety of technological strategies for strengthening the connections from NICU to early intervention services.
Connecting Health Care with Early Intervention
- Raise the standards for electronic health records (EHR). Connecting health care and early intervention records can significantly speed up the referral and evaluation process. Early intervention coordinators noted the importance of this capability, yet EHR systems may not sufficiently support the healthy development of preterm infants if they do not include corrected age or developmental tracking features like the inclusion of video recordings of preterm infant movements.20 And while state early intervention coordinators expressed interest in direct linkage of referrals to EHR systems, only 8 percent reported having that capability in a 2022 study.21
- Leverage EHR capabilities where possible. Electronic health records can prompt providers like pediatricians to ask families with babies who should qualify for early intervention if they have been connected yet, and if not, whether they would like to be referred. Yet EHR systems are not a solution for every problem, and providers can experience “nudge fatigue” from overreliance on them for reminders and prompts. Adding new features to already complex systems should be carefully considered. One provider we spoke with pointed out that “nudge fatigue” is a particular problem when providers are prompted to do things where they have no particular expertise or control, and when the action is repetitive or feels pointless. Involving them in the design of such nudges may help avoid that fatigue and align solutions to the actual problems they experience in their practices. One state’s city-based referrals were configured to connect all city hospitals’ electronic medical records with early intervention programs. It was not a small undertaking, as permissions had to be navigated with each participating hospital. However, configuring these systems up front reduces burden for NICU and early intervention staff in the long run. Early intervention programs do not have to wait for medical records from the NICU and can quickly access medical histories, easing the burden on families who would otherwise have to coordinate records transfers and retell medical history information to multiple providers.
- Implement electronic referral and centralized enrollment when possible. Integrating screening, consent, and referral forms in several languages into electronic health records helped NYC Health + Hospitals increase general referrals to early intervention by 30 percent and reduce the average age of enrollment by six months. Another state offers e-referrals as one of five referral avenues. The e-referral option shares relevant information from an infant’s medical record from the NICU directly with the early intervention program’s Salesforce system and increases the visibility of an infant’s status in the referral process.
- Loop eligibility criteria into well-baby visits so pediatricians can focus on parent education. Automating or integrating some of the complex program requirements into prescreening tools or electronic health records could help pediatricians focus their time on educating families about what early intervention services could do for their children, rather than wrestling with diagnostic criteria. Programs like StreetCred are designed to better connect children and families with financial coaching and a suite of services that can help support child wellness and healthy development, including tax preparation, paid family and medical leave, and supports like the Women and Infants, and Children (WIC) program and the Supplemental Nutrition Assistance Program (SNAP). Children in families that are eligible for services like SNAP and WIC may also be at higher risk of developing a delay, particularly in households experiencing poverty.22 Integrating developmental resources into primary care along with financial support helps address multiple household needs. Since infants typically have seven or more primary care visits in the first year of life, services like this would provide regular touchpoints with helpful services for families regardless of NICU involvement.
Connecting Family with Early Intervention
- Use smartphones to reach families. Family email, text message, and smartphone access have been associated with increased enrollment in early intervention programs following NICU discharge.23 For general identification of infants and toddlers eligible for early intervention, the Text4Baby program sent developmental screening questions to mothers with low incomes via text message and sent follow-up texts with health resources.24 A study of this initiative found high acceptability and usability of this intervention.25 Los Angeles successfully used a call center to connect families of toddlers with early care and education coordination, including developmental services, increasing both referral and enrollment. Though the intervention was limited to children over 12 months, it could be piloted with younger babies as well.26
- Other ehealth technology options, such as apps and social media, can support families. Focus groups of an early intervention referral and family engagement app found that families found it useful to have an app provide clear communication that explained the fundamentals of services, let them give feedback on their experience, and helped them track their progress through the system.27 While “low-touch” approaches like this may seem like budget-friendly options, they require ongoing commitment and technical upkeep to remain usable and compatible with a range of devices and systems.
- Offer telehealth as an option (but not the only option). The COVID-19 pandemic led states to use telehealth for administering early intervention services.28 State programs still use telehealth to deliver services to some families in rural areas. One program administrator noted that while in her experience most families prefer home-based service delivery, others prefer telehealth for a multitude of reasons. Though guidance often recommends home-based service delivery, this may not always be culturally responsive, and it is important to respond to family preferences that may evolve over time.
Structural Fixes
Early intervention was established by a federal law, Part C of the Individuals with Disabilities Education Act (IDEA), but is largely subject to implementation differences from state to state. IDEA Part C is unlikely to be amended to solidify local NICU procedures—it does not even establish a consistent list of qualifying conditions across states. That said, federal and state legislation has been introduced to improve the NICU experience for families and to better connect NICU infants to services through discharge planning.
Legislative Approaches to Smooth Family Experience
- Support paid family and medical leave at the state level. Colorado became the first state to approve additional paid family and medical leave to support families with infants in NICU. Starting in 2026, 12 additional weeks of paid family leave will augment Colorado’s existing Family and Medical Leave Insurance (FAMLI) program to support these infants and their families. This is an excellent benefit for NICU families in general, and it also provides another touchpoint for cross-benefit referral or enrollment in other services like early intervention. If families are applying for paid leave to support their families during NICU stays, they may also benefit from referral to other supportive services at that time. In Illinois, a bill introduced by State Senator Bill Cunningham extends the amount of unpaid but job-protected leave the parents of infants in NICU can take to spend time with their babies. Under this measure, employees of companies with 16 or more workers will be eligible for either 10 or 20 days of NICU-related leave depending on the size of their companies. Families will likely need much more time, and paid leave is optimal, but it is a small yet meaningful step in the right direction.
- Improve NICU discharge procedures with early intervention information and connections. Another Illinois bill, introduced by State Representative Janet Yang Rohr, herself a NICU parent, stipulates that early intervention education and written referrals for eligible infants be included in hospital discharge of infants from NICU. Signed into law in August, this bill aims to create more consistency in early intervention referrals at NICU discharge in the state of Illinois.
- Advance a “NICU Bill of Rights” in Congress. Representatives Erin Houchin and Morgan McGarvey introduced a resolution expressing support for a “NICU Bill of Rights” that aims to promote family-centered care, strengthen informed consent, support mental health for families, and improve discharge planning. While supportive programs like early intervention and paid family and medical leave are not explicitly mentioned, the text does call for family-inclusive policies and comprehensive discharge planning.
Systems Thinking to Deliver Services More Efficiently
The uncomfortable truth remains that even in a best-case scenario where all procedural, cultural, and tech fixes are implemented, enrolled families would still run into a wall of provider and funding scarcity. The Government Accountability Office reported that early intervention state coordinators consistently identified staff shortages and program capacity as their biggest challenge, and states that open up eligibility run the risk of rationing care to children who are already being served.29 Still, ignoring the need won’t help.
The increasing number of high-risk pregnancies, preterm births, and improving survival rates of very preterm infants will mean higher demand for early intervention services for infants at risk of delays and toddlers who are experiencing them.30 Underinvestment in these services will compound service gaps over time. But the current federal and state budget environments across early childhood programs are not conducive to expanding services, despite the widespread bipartisan demand among families for better support. States opting for a systems-thinking approach—for example, orienting supports around the experience of having or raising a child rather than around a particular program or problem—can leverage other federal programs supporting maternal and child health to maximize benefits to families with current capacity.31
- Pursue better coordination of early childhood programs to create additional family touchpoints for early intervention. For example, Maternal, Infant, and Early Childhood Home-Visiting (MIECHV) programs, including Nurse-Family Partnership, provide services to many families eligible or enrolled in early intervention. Yet in 2016, only one quarter of states reported enrollment coordination between MIECHV and early intervention programs.32 For instance, in one state, fewer than half of program participants discussed early intervention with home visiting staff, about one quarter were referred, and only 10 percent of those referred connected to early intervention services.33 Strengthening referral and enrollment practices in these related community-based programs could efficiently increase early intervention connections.
- Leverage authority built into the early intervention system to explore partnerships. Part C is collaborative by design and lends itself to interagency work. According to the Early Childhood Technical Assistance Center (ECTA), “Lead agency staff are often asked to participate in many state-level collaborative activities designed to enhance the statewide system of services for all young children and families. The participation of staff in these collaborative efforts is extremely important.” ECTA notes that section 34 CFR §303.605 “specifically mentions collaboration” with the State Advisory Council on Early Education and Care and MIECHV programs.34
- Look for examples where program coordination has proven results. Home visiting programs such as Help Me Grow South Carolina have successfully integrated the federal “Learn the Signs. Act Early.” developmental monitoring program and could use that integration to strengthen referral and enrollment to early intervention. In another study, participants in Massachusetts’ Welcome Family home visiting program had greater odds of receiving IFSPs relative to the comparison group.35
- Coordinate with state-based perinatal quality collaboratives (SPQCs). These organizations work to improve maternal and newborn care and may be avenues to address connection of infants to early intervention in the future. According to a 2017 study, “While each SPQC uses approaches suited to its own context, several themes are common to the goals of all SPQCs, including developing obstetric and neonatal partnerships; including families as partners; striving for participation by all providers; utilizing rigorous quality improvement science; maintaining close partnerships with public health departments; and seeking population-level improvements in health outcomes.”36 These SPQCs have also coordinated in cross-state collaborations to maximize their impact across broader regions.
- Leverage improved implementation of Medicaid’s pediatric benefit, Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) for children. Of the 540,000 children currently receiving early intervention services, about half are also enrolled in Medicaid. Medicaid covers comprehensive screening, testing, and any follow-up treatment services for enrolled children. Using EPSDT to its full potential may help shore up additional resources to help identify children for early intervention services, helping to reduce some of the logistical challenges of Child Find efforts. If states ensure all medically necessary early intervention services are also reimbursed by Medicaid for enrolled children, that could free up additional federal or state resources to strengthen the screening and referral systems. States like Washington are working to ensure all early intervention providers are recognized by Medicaid plans, for example. The Bipartisan Safer Communities Act of 2022 requires the Centers for Medicare and Medicaid Services (CMS) to more actively monitor state implementation of EPSDT, resulting, to date, in updated CMS guidance, including a section on children with specialized needs.
- Provide federal guidance to states that clarifies which babies are included in automatic eligibility criteria. Currently each state chooses among automatically eligible conditions, leaving high variability among states and causing confusion about which conditions are included.
Citations
- Alison Little et al., “Understanding Barriers to Early Intervention Services for Preterm Infants: Lessons From Two States,” Academic Pediatrics 15 (2015): 430–438, source.
- Litt et al., “Ensuring Optimal Outcomes for Preterm Infants After NICU Discharge,” 146, source.
- Susan Hintz et al., “Referral of Very Low Birth Weight Infants to High-Risk Follow-up at Neonatal Intensive Care Unit Discharge Varies Widely Across California,” Pediatrics, 166 (2015): 289–95, source.
- Sandhya Brachio et al., “Improving Neonatal Follow-Up: A Quality Improvement Study Analyzing In-Hospital Interventions and Long-term Show Rates,” Pediatric Quality and Safety, 23 (2020): e363, source.
- Ashwini Lakshmanan et al., “Connecting to Early Intervention Services After Neonatal Intensive Care Unit Discharge in a Medicaid Sample,” Academic Pediatrics 22 (2022): 253–262 source.
- Jessica Trenkle et al., “Project Initiate: A Clinical Feasibility Trial of Equitable Access to Early Neurodevelopmental Therapy,” Clinical Medicine 13 (2024): 7681, source.
- Lakshmanan et al., “Connecting to Early Intervention Services After Neonatal Intensive Care Unit Discharge in a Medicaid Sample,” source; Smith, Love, and Goyer, “NICU Discharge Preparation and Transition Planning,” source.
- Emily Feinberg et al., “Effect of Family Navigation on Participation in Part C Early Intervention,” Academic Pediatrics 23 (2023): 904–912, source.
- Lakshmanan et al., “Connecting to Early Intervention Services After Neonatal Intensive Care Unit Discharge in a Medicaid Sample,” source.
- Lea Redd et al., “A Silver Lining for Neonatal Intensive Care (NICU) Graduates: Coordinated Services from 0-6 Years,” International Public Health 10 (2018): 325, source.
- Brian Barger et al., “State Variability in Diagnosed Conditions for IDEA Part C Eligibility,” Infants and Young Children 32 (2019): 231–244, source.
- Little et al., “Understanding Barriers to Early Intervention Services for Preterm Infants,” source.
- Sandhya Brachio et al., “Improving Neonatal Follow-up: A Quality Improvement Study Analyzing In-Hospital Interventions and Long-Term Show Rates,” Pediatric Quality and Safety 23 (2020): e363, source.
- Yadav, Phelps, and Squires, “Knowledge of Established Conditions List and Associated Policies and Procedures Among Pediatricians and Early Intervention Personnel,” Developmental and Behavioral Pediatrics 76 (2025): 64–70, source.
- Lakshmanan et al., “Connecting to Early Intervention Services After Neonatal Intensive Care Unit Discharge in a Medicaid Sample,” 22, source; Brachio et al., “Improving Neonatal Follow-Up,” source.
- Theiju Sebastian et al., “Improving Access to Neurodevelopmental Resources for NICU Graduates,” Perinatology 44 (2024): 578–580, source.
- Roberta Pineda et al., “The Baby Bridge Program: A Sustainable Program That Can Improve Therapy Service Delivery for Preterm Infants Following NICU Discharge,” PLoS One 15 (2020): 1–12, source.
- Smith, Love, and Goyer, “NICU Discharge Preparation and Transition Planning,” source.
- Jonathan Litt et al., “Ensuring Optimal Outcomes for Preterm Infants After NICU Discharge: A Life Course Health Development Approach to High-Risk Infant Follow-Up,” Children (Basel) 11 (2024): 146, source.
- Sanders et al., “Early Intervention Referral Information, Transmission, and Sources,” source; Kevin Dufendach, Christoph Lehmann, and S. Andrew Spooner, “Special Requirements of Electronic Health Record Systems in Pediatrics: Clinical Report,” Pediatrics 154 (2024): e2024068509, source.
- Sanders et al., “Early Intervention Referral Information, Transmission, and Sources,” source.
- Sara Johnson, Jenna Riis, and Kimberly Noble, “State of the Art Review: Poverty and the Developing Brain,” Pediatrics 137 (2016): 20153075, source.
- Nicole Flores-Fenlon et al., “Smartphones and Text Messaging Are Associated With Higher Parent Quality of Life Scores and Enrollment in Early Intervention After NICU Discharge,” Clinical Pediatrics 58 (2019): 903–911, source.
- Brian Suffoletto, “Deceptively Simple Yet Profoundly Impactful: Text Messaging Interventions to Support Health,” Medical Internet Research 26 (2024): e58726, source.
- Pamela Ryden Johnson et al.; “Usability and Acceptability of a Text Message-Based Developmental Screening Tool for Young Children: Pilot Study,” JMIR Pediatrics and Parenting 2 (2019): e10814, source.
- Bergen Nelson et al., “Early Childhood Care Coordination Through 211: A Randomized Clinical Trial,” Pediatrics 154 (2024): e2023065232, source.
- Liliana Wagner, “Development of an App for Tracking Family Engagement With Early Intervention Services: Focus Groups and Pilot Evaluation Study,” JMIR Human Factors 10 (2023): e45957, source.
- Jackson Kwok et al., “Impact of the COVID-19 Pandemic on Early Intervention Services Use Among Children with Developmental Disabilities,” Pediatric Advance Research 3 (2024): 1–9, source.
- Government Accountability Office, “Special Education: Additional Data Could Help Early Intervention Programs Reach More Eligible Infants and Toddlers,” GAO-24-106019 (2023): 19, source.
- Eran Bornstein et al., “Concerning Trends in Maternal Risk Factors in the United States: 1989–2018,” EClinicalMedicine (2020): 29–30, source; Joyce Martin and Michelle Osterman, “Shifts in the Distribution of Births by Gestational Age: United States, 2014–2022,” National Vital Statistics Report 73 (2024): 1–11, source; “Survival of the Tiniest,” National Institute of Child Health and Human Development, 2022, source.
- Kate Milner et al., “No Time for Business as Usual: Can Systems Thinking Help Us to Accelerate Recovery for Early Child Development?,” BMJ Global Health 8 (2023), source.
- Abby Winer Schachner et al., “Early Intervention and Home Visiting State Systems: Partners in the Making,” presented at the Conference on Research Innovations in Early Intervention in San Diego, California (February 2016), source.
- Jessica Goldberg et al., “Getting to the Warm Hand-Off: A Study of Home Visitor Referral Activities,” Maternal and Child Health 22 (2018): 22–32, source.
- “Part C of IDEA,” Early Childhood Technical Assistance Center, April 3, 2025, source.
- Chie Kotake et al., “Improving Connections to Early Childhood Systems of Care via a Universal Home Visiting Program in Massachusetts,” Children and Youth Services Review 150 (2023), source.
- Munish Gupta, Edward F Donovan, and Zsakeba Henderson, “State-Based Perinatal Quality Collaboratives: Pursuing Improvements in Perinatal Health Outcomes for All Mothers and Newborns,” Seminars in Perinatology 41 (2017), 195–203, source.
Conclusion
Even though our team is not new to the early childhood space, we were still surprised to learn about the complexity and challenges in delivering early intervention services, both to low birth weight and preterm babies who might be automatically eligible and more broadly across the population. Early intervention is a critical support for the infants, toddlers, and families who need its services, but successful implementation is hampered by procedural, cultural, technological, and structural barriers. On the structural point, it is critical to highlight the extent to which the Individuals with Disabilities Education Act (IDEA) Part C funding has lagged over time in relation to the number of children served by the program. IDEA Part C has multiple legally mandated components at the federal level, one of which is for IDEA Part C funds to serve as the “payor of last resort.” States that want to serve more children—including infants—do so on their own dime and largely at their own risk. Each state must weigh the benefits of reaching more children against the cost of providing timely service as required by law.
In general, the United States operates in a scarcity mindset when it comes to serving our youngest children and their families. This country chronically underspends on early care and education compared to its Organization for Economic Cooperation and Development (OCED) counterparts.1 This scarcity too often results in rationing of care: difficult eligibility processes, service delays, and wait lists for families looking for support while raising young children. State administrators face difficult decisions when considering who to prioritize, and in many cases, they have insufficient evidence for decision-making. The questions over the appropriate dosage, duration, and type of services that will benefit developing children are far from settled, and this report does not provide a definitive answer to those questions.2
What is very clear is that states seeking to connect families of infants with neonatal intensive care unit (NICU) stays to early intervention services have plenty of opportunities to do so, largely through the cultural, procedural, structural, and technological improvements surfaced in this report. In many cases, solutions focus on bridging the gaps between what is health care and home care: in other words, strengthening the connection between the highly clinical work of resuscitating fragile infants and the family-centered, ongoing developmental support they will need at home to help them develop and thrive.
The challenge of integrating these two types of care is not unique to early intervention—transitions from hospital to home are often challenging.3 And within the early intervention space, the disconnect is not isolated to NICU transitions. Indeed, better integration of developmental screenings, early intervention referrals, consent forms, service plans and records, and pediatric electronic health records would be likely helpful to all children and their families, not just automatically eligible infants, and not even just children who are currently enrolled in services. Building additional capabilities into the existing system will help programs like early intervention operate more efficiently and effectively if and when they are sufficiently funded to fully meet the needs of children and families.
Citations
- “OECD Family Database: Public Spending on Child Care and Early Education,” Organisation for Economic Cooperation and Development,” 2023, source.
- Batya Elbaum and Seniz Celimli-Aksoy, “Developmental Outcomes of Children Served in a Part C Early Intervention Program,” Infants & Young Children 35 (2022): 3–19, source.
- Mahiyar Nasarwanji et al., “Identifying Challenges Associated With the Care Transition Workflow From Hospital to Skilled Home Health Care: Perspectives of Home Health Care Agency Providers,” Home Health Care Services Quarterly 34 (2015): 185–203, source.
Appendix
New America is a “think and action” tank that is dedicated to realizing the promise of America in an era of rapid technological and social change. Within New America, multiple programs focus on issues related to family and economic security and well-being, including access to early care and education programs for families with young children.
New America’s Early and Elementary Education Policy team works to help ensure that all children, including young children with disabilities and developmental delays, have access to high-quality early learning opportunities starting at birth that prepare them to thrive in school and life. We aim to help realize this new system by conducting policy research and analysis, putting forth innovative policy recommendations, and disseminating new ideas to a variety of audiences, including federal and state policymakers.
The New Practice Lab’s theory of change centers on listening to the people who are most impacted by public programs: the people who they are meant to serve, and the people who deliver them. Our portfolio includes programs that support the family unit, working parents, and their children: tax credits, paid leave, and early education and child care. We believe that by bridging the gap between policy design and implementation, we can create a feedback loop that will help more families now—and create the conditions for more usable services and programs going forward.
Together, we embarked on an eight-week discovery sprint to better understand the barriers to early intervention that could lead to service gaps among high-risk children who may be missing out on important services, even when factors such as very low birth weight or low gestational age may make them automatically eligible.
Our team was curious to learn more about procedures for automatically connecting eligible babies to early intervention services, and to better understand provider, administrator, and family perspectives on what’s working well and what’s not. We were also interested in determining how widespread practices may be across hospital systems and geographies, and the extent to which learning and solutions may transfer across localities.
Methodology
Our discovery research primarily consisted of three lanes of effort:
- Learning more about current practices, gaps, and drivers by reviewing academic literature and other documentation about high-risk infants, their families, and their treatment and service transitions through their early years;
- Analyzing publicly available data about early intervention and related early childhood programs related to prenatal care, NICU stays, and perinatal care for high-risk infants; and
- Conducting 14 interviews with experts in the fields of neonatology, public policy, early intervention, social work, and perinatal health.
We did not engage with families directly at this point due to the time-limited nature of this discovery sprint and additional capacity requirements for conducting trauma-informed research with this population. To collect an initial reading of these perspectives, we relied on the perspectives of expert interview subjects in our third workstream, reviewed qualitative research describing family perspectives, and read postings on parent message boards.
What Is Early Intervention, and How Do Families Enroll?
Early intervention is an important and much-used program in the suite of federally supported early childhood services. Among the “core four” program areas identified in a previous brief, early intervention served 441,515 children in 2023, though this likely reflects a limited “point in time” count and not the full number of infants and toddlers who receive service in a year. This is better reflected by a cumulative count, such as the one provided by a birth cohort study conducted by the Infant and Toddler Coordinators Association.
Many of the best-known federal programs such as Head Start, child care subsidies, and Women, Infant, and Children (WIC), are “means tested,” meaning there are income limits governing who can apply. Unlike means-tested programs, enrollment in early intervention (EI) services requires several steps: (1) identification via Child Find, (2) referral, (3) evaluation, (4) service planning, and (5) service delivery.
There are several considerations:
- Each step has its own set of federally mandated requirements that are then implemented at the state level in different ways.
- We do not exhaustively describe each step of the early intervention process here, but we explain the general pathway to enrollment along with potential pain points in each step to highlight why automatic eligibility and enrollment are important tools for families and providers.
- Finally, racial, demographic, and geographic disparities in access to health care persist and are woven throughout each step of the early intervention process, with significant impacts. Solving for these access disparities must remain a research priority to get the best outcomes for children and families who face the biggest barriers to help that they are entitled to receive.
Identification
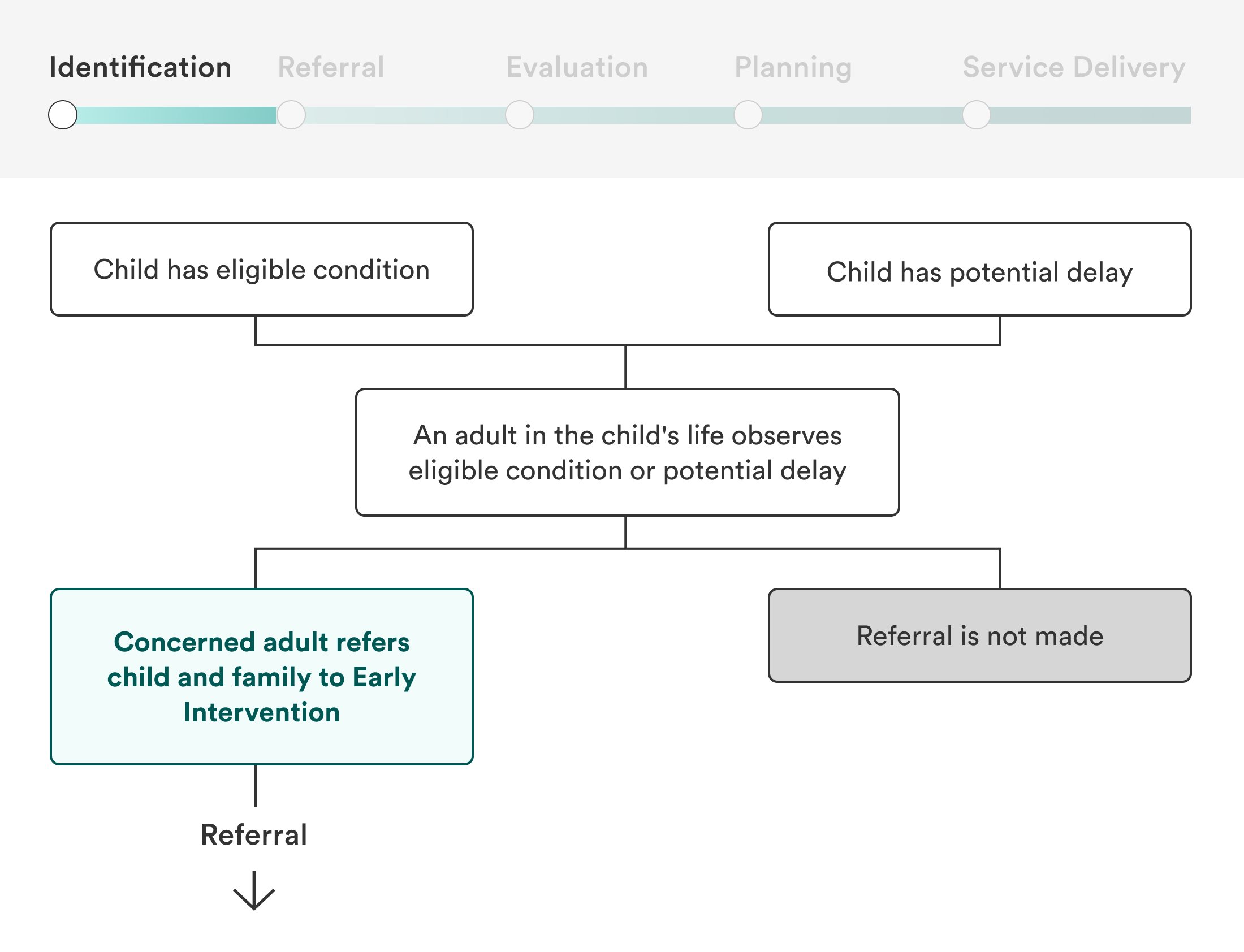
In the Child Find identification process required by IDEA Part C, children are eligible if they are under the age of three and have either observed developmental delays or eligible conditions with a high probability of developmental delay.
Even though infants are eligible, many are not identified for referral until they are 18 months or older. While some younger babies are diagnosed with delay or conditions very early and are quickly identified in Child Find, others have undiagnosed conditions that are difficult to pinpoint and will not be identified until later.
Preterm birth and low birth weight are easily observable characteristics that are strongly associated with risk of developmental delay. Many states allow them as eligible conditions, meaning their families can bypass more difficult steps to enroll. In states where this is not allowed, preterm and low birth weight babies will not be flagged during the Child Find process unless they have other eligible conditions.
Referral
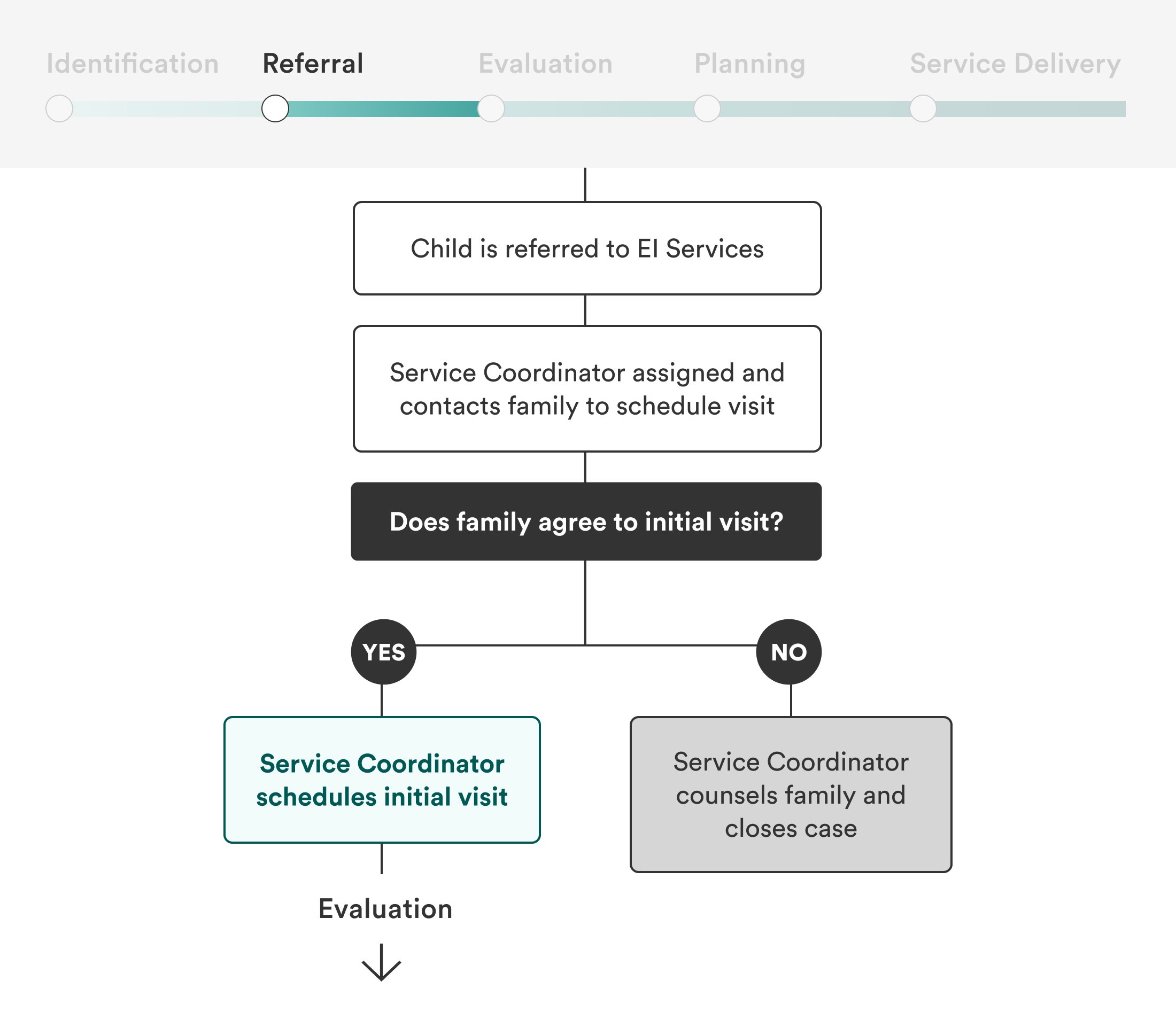
Anyone can refer infants and toddlers to early intervention services. For babies in the NICU, referrals are often dependent upon a doctor, social worker, or other hospital member providing information to families. Pediatricians who see NICU babies following hospital discharge can also make referrals. Once babies leave the hospital setting for the first time, however, referrals become more challenging and less likely, as qualifying presentations can become more subtle and difficult to diagnose.
Referral processes vary widely by state, county, and hospital, and understandings of referral criteria may vary even more. A misconception persists among medical providers and early educators that a child must already have a developmental delay in order to qualify for early intervention, when in fact children with certain medical conditions qualify simply with “high probability of resulting in developmental delay.”
When referrals based on low birth weight or prematurity are allowed but do not happen, families and infants lose time to access important services in the earliest possible stages of children’s development. Families who have not received appropriate information about their children’s conditions and the availability of services may not agree to an initial visit.
Evaluation
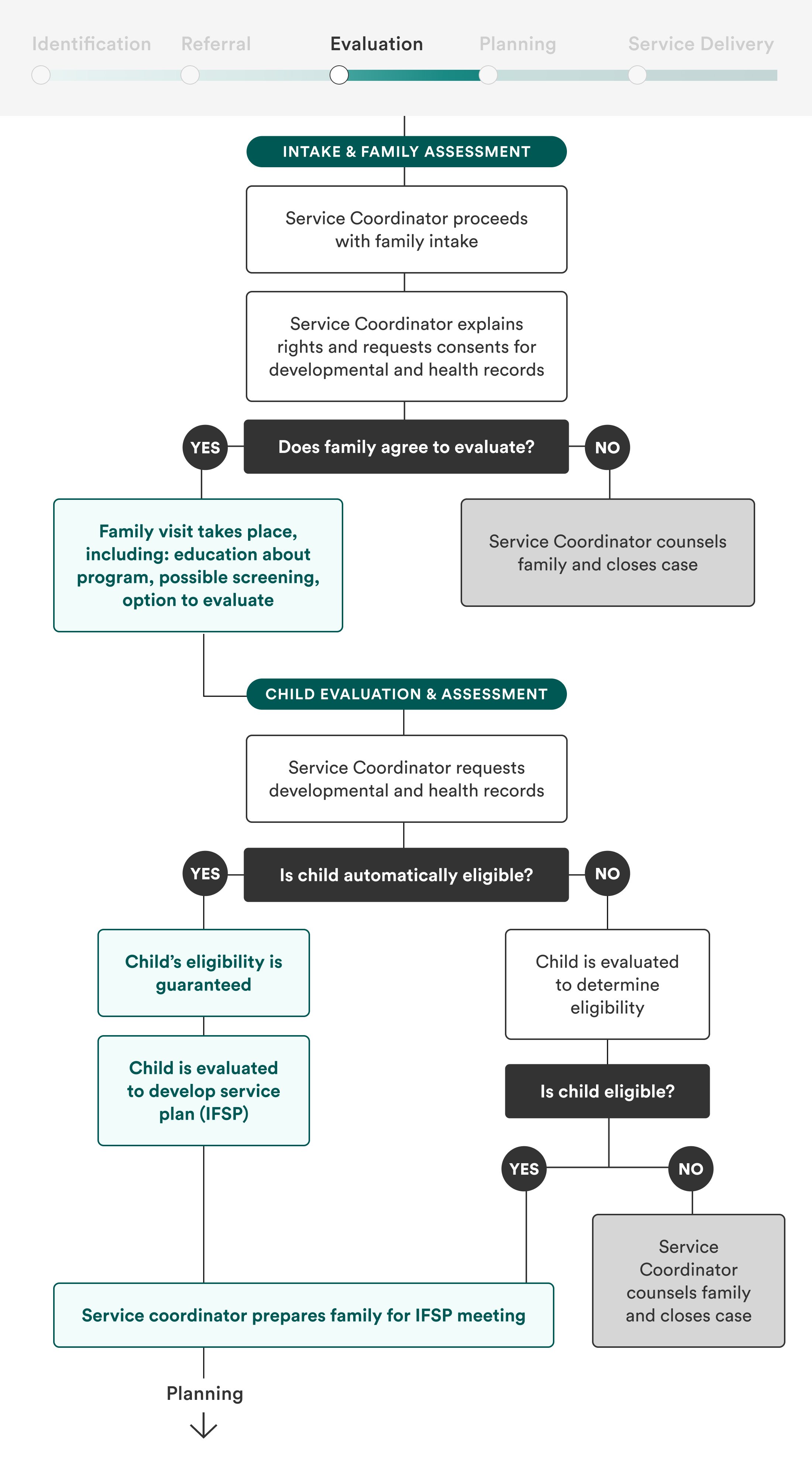
After being referred, the baby and their family must be evaluated further, including a meeting with the family to assess their routines, home environment, and developmental concerns, as well as an evaluation of the child’s developmental milestones. It’s a process that requires time, effort, and skill on behalf of the evaluators, and one that can be complicated by parental hesitation, stigma, language barriers, transportation barriers, and more factors.
Infants and toddlers that were not immediately identified and referred must first be evaluated by a specialist in order to be eligible, a process that can take weeks—a significant amount of time in a young child’s life. Evaluation services may be scarce and inconvenient for families to access.
To properly connect infants with appropriate therapies, evaluation will need to occur whether infants are automatically eligible for services or not. However, automatic eligibility for low birth weight and preterm infants exiting NICU will counterbalance the time-consuming and potentially stressful experience of evaluation with a guarantee of services.
Planning
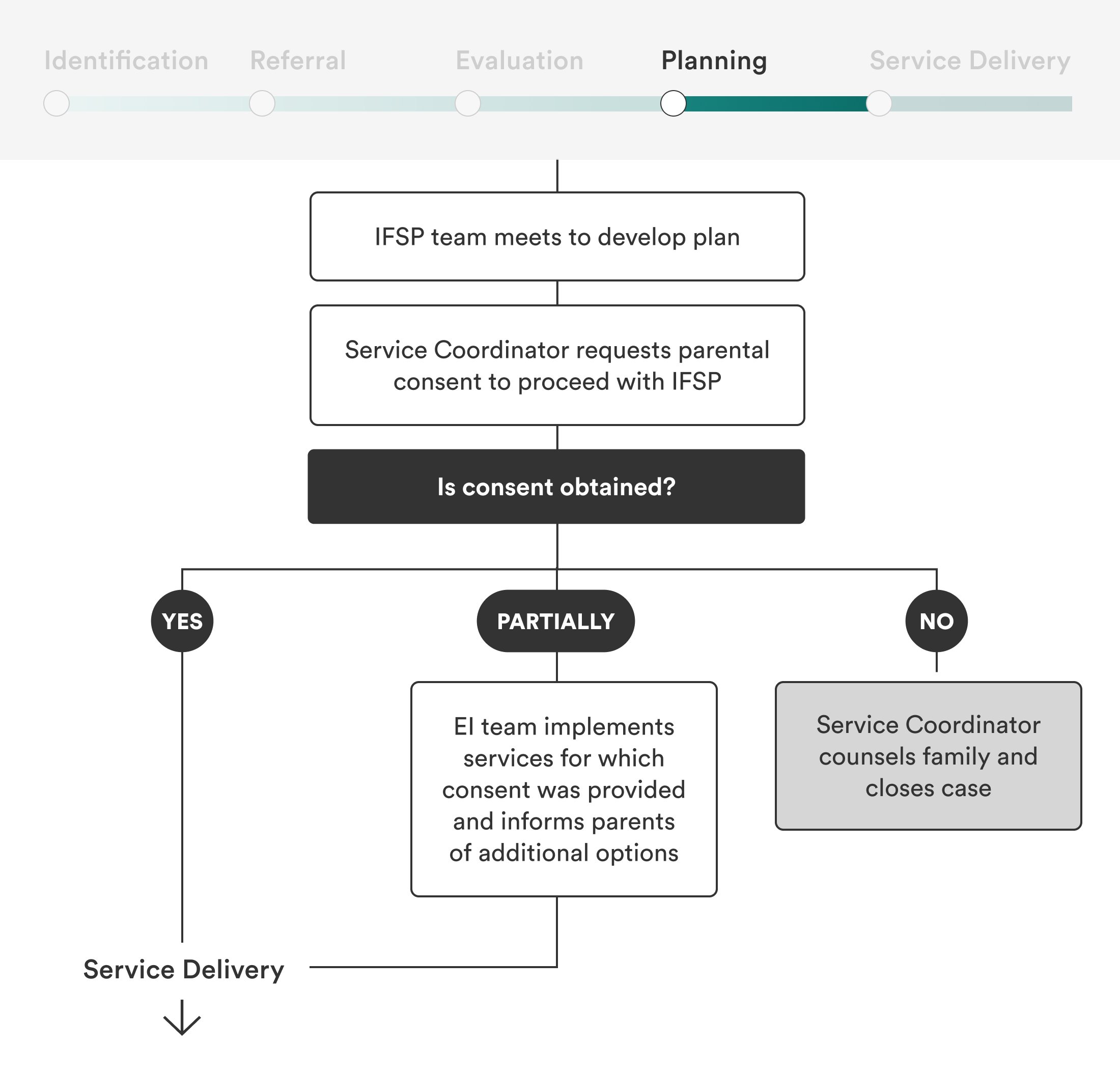
The early intervention team and family collaboratively develop a roadmap for services to support the child’s development known as an Individualized Family Service Plan (IFSP). The plans should include parent priorities, functional outcomes, appropriate services, and timelines for service. Once the IFSP is in place and consent is obtained, services can commence.
IFSPs are important (and required!) documents for coordinating early intervention services and will need to be in place whether or not a child is automatically eligible for services. Even though preterm and low birth weight infants will likely need some of the same early intervention services and may have even received some in NICU (speech therapy for feeding, for example, is common), their needs will vary and services should be targeted to meet families where they are. Since IFSPs are reevaluated annually, the longer infants are in the program, the more opportunities there will be to reassess and tweak service plans as needed.
Service Delivery
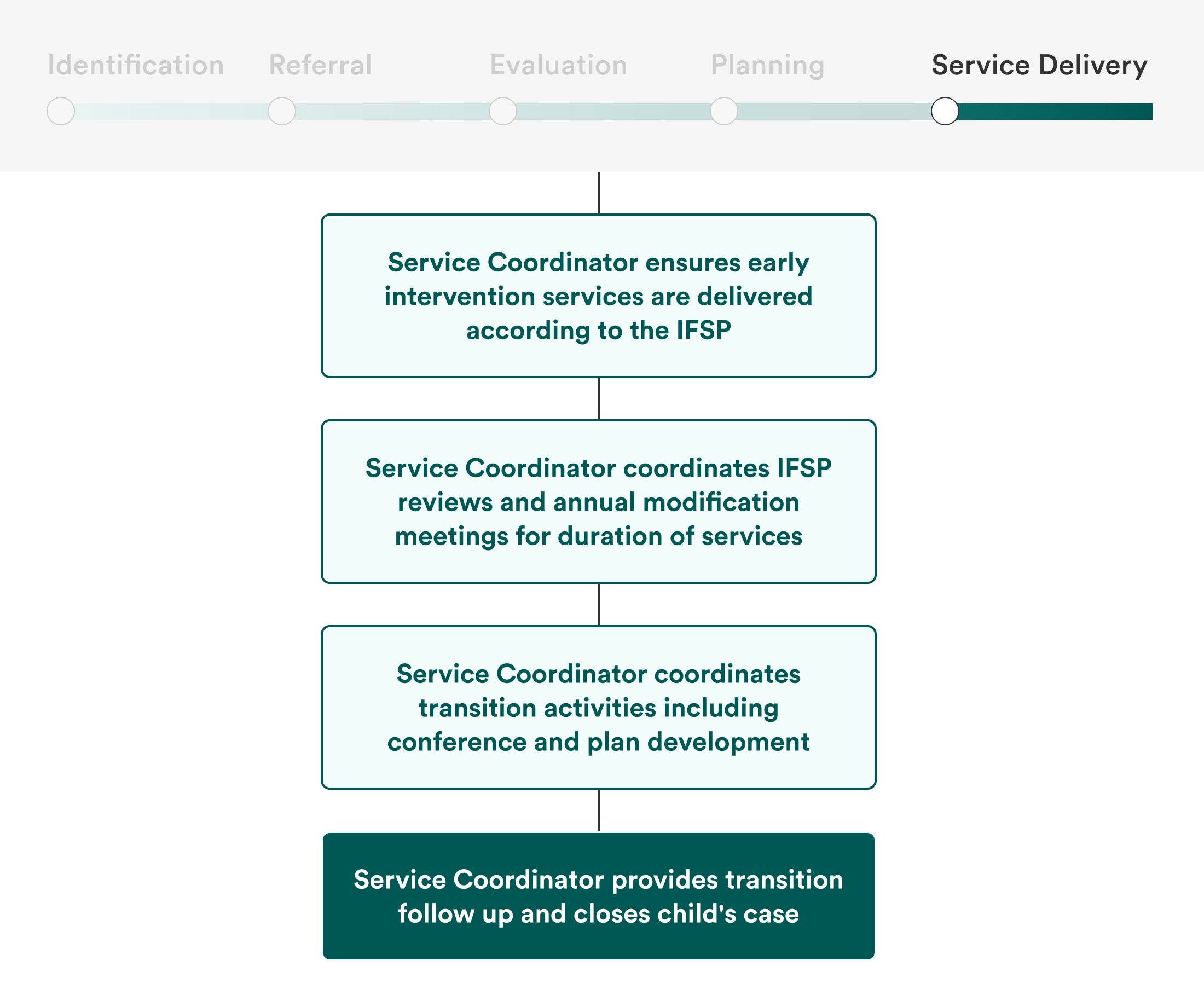
Once approved for services, families will need to be connected to appropriate provider such as occupational, speech and language, and physical therapists.
Automatic eligibility can enroll families more quickly, which is crucial for the populations that this approach would cover. Yet even with the advantage of an expedited process through automatic eligibility, the early intervention workforce shortage across the United States may make it difficult for families to find available providers. Furthermore, families with infants and toddlers have limited time and energy. Lower-income families lack cash and basic needs like food, diapers, housing, and reliable transportation, and may have demanding or irregular work schedules, language barriers, or other challenges that make it difficult to attend appointments consistently. Policies must address the chronic early intervention workforce shortage and the overall accessibility of early intervention programs in order to more comprehensively improve the system.
More About the Authors

Carrie Gillispie
Project Director, Early Development & Disability

Sarah Gilliland
Senior Policy Manager, New Practice Lab
Programs/Projects/Initiatives
Related


Closing Early Intervention Service Gaps to Infants is Both Policy and Practice

Fact Sheet: Care Economy Investments in Build Back Better