
Part 2: High-Intensity Caregiving and/or Parenting by Black Men
Eighty-six percent of Black men who are High-Intensity Caregivers and/or Parents (HICP) have helped adults with hands-off tasks (instrumental activities of daily living), and almost two-thirds (65 percent) have provided hands-on care (basic/physical activities of daily). More Black male HICPs than white male HICPs performed hands-on medical or nursing tasks.1
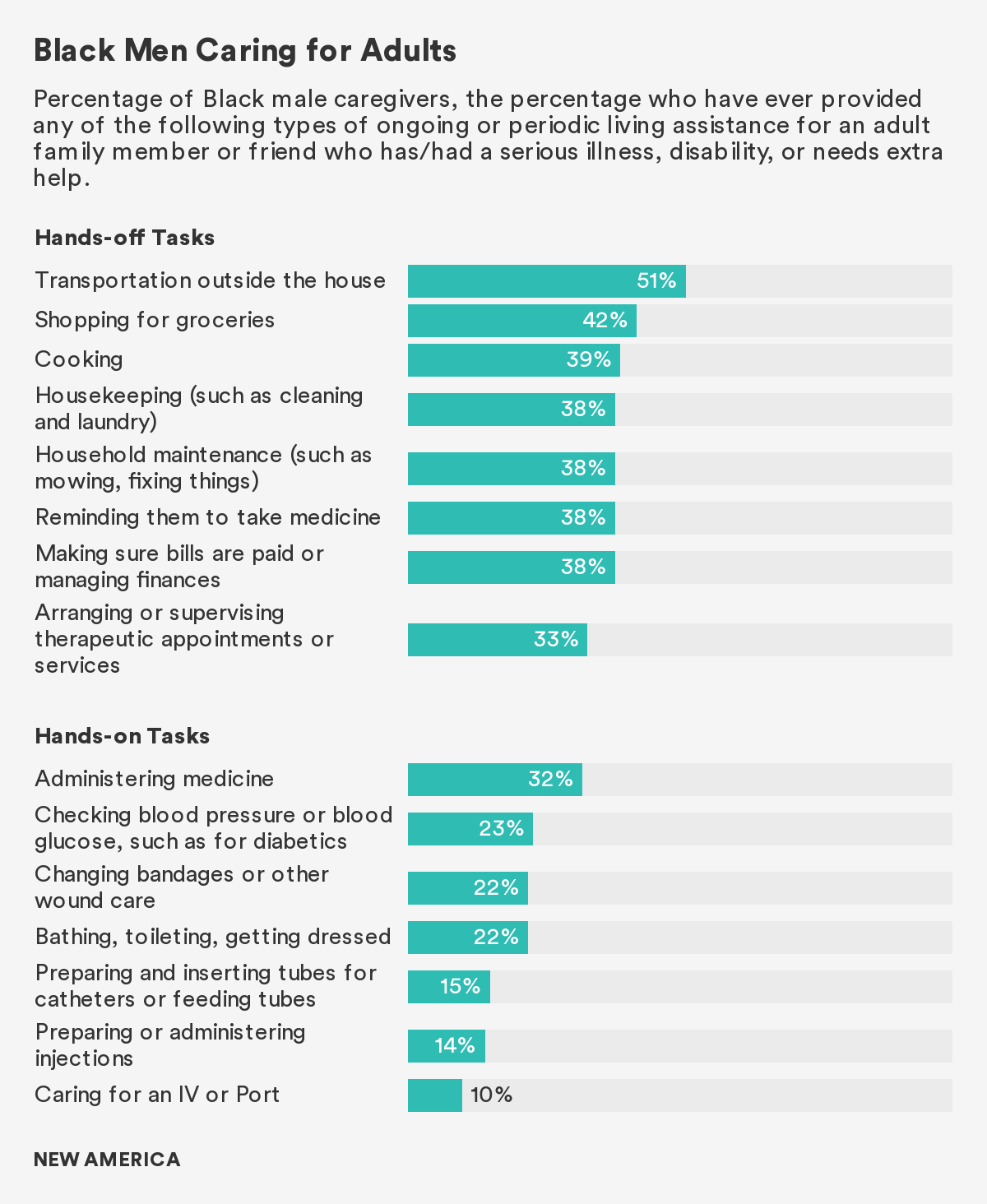
A majority of Black male HICPs play an active role in caring for adult family members or friends who have or have had a serious illness or disability. The vast majority (86 percent) say that they have supported adult care recipients with instrumental activities of daily living, like shopping for groceries, housekeeping, cooking, making appointments, paying bills, reminding care recipients to take medication, and providing transportation. Additionally, almost two-thirds (65 percent) have performed tasks that meet the medical needs of care recipients.
Medical or nursing tasks are those activities that resemble the paid work of in-home health aides and professional long-term care providers who receive some form of professional training. Fifty-three percent of Black men caring for adults have administered medication, 40 percent have performed blood checks or assisted with bathing, and about a quarter have performed injections.
Black male HICPs are among the 58 percent of adults in the United States providing nursing level assistance to adults they care for.2 Research from AARP’s 2019 report, Home Alone, finds that caregivers providing this level of hands-on care often do so with little support from the healthcare infrastructure, lack training, and face emotional challenges associated with the role.3 Moreover, the study finds that caregivers who perform medical or nursing level tasks report increased feelings of worry, stress, and financial strain.
Although half of all Black male HICPs find this work more stressful than other kinds of work they perform, 89 percent find caregiving satisfying, and 87 percent feel respected in their roles.
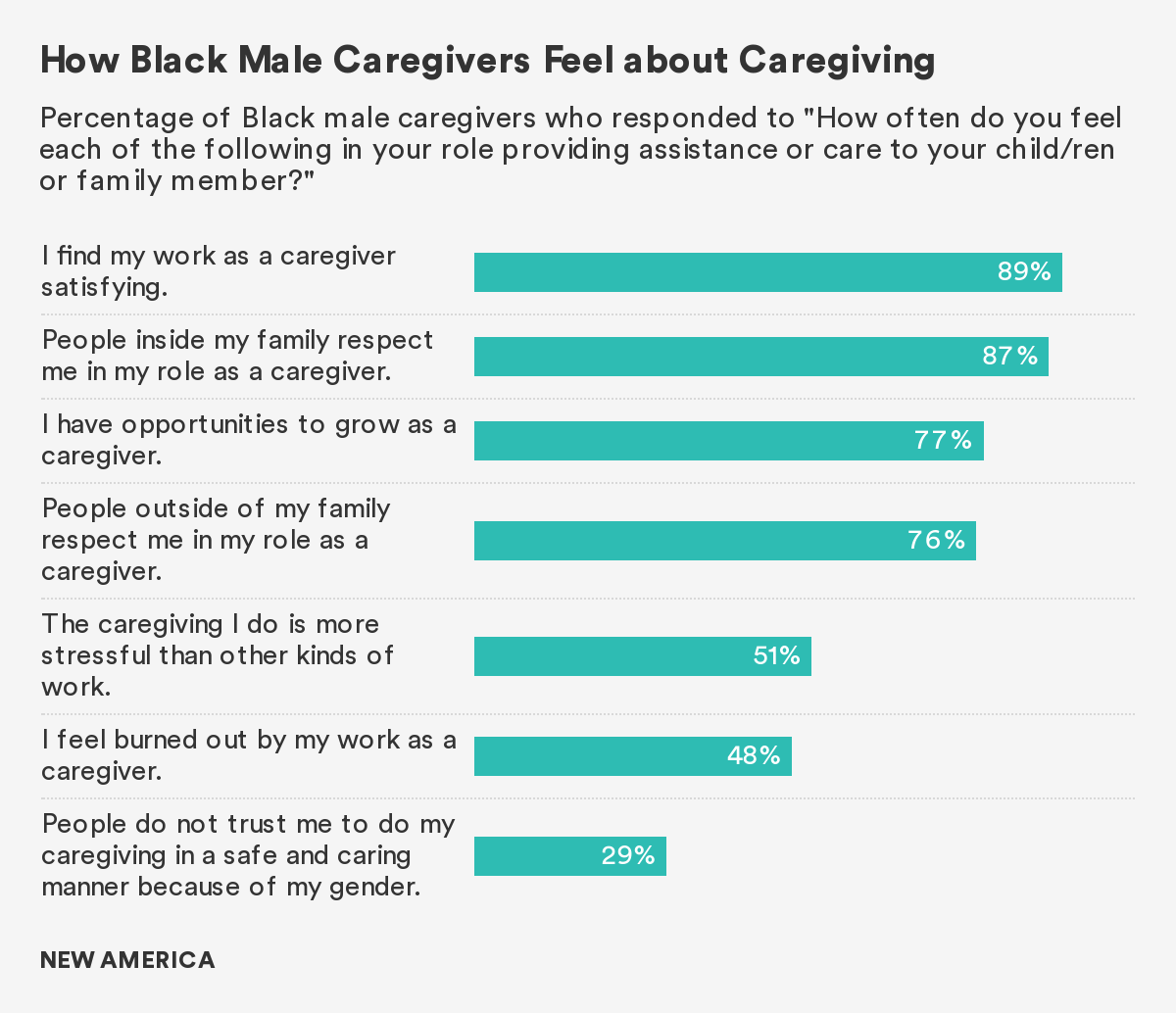
Providing care can be a gratifying experience. The vast majority of Black male HICPs who have cared for a child with special needs or an adult have had a positive caregiving experience. In this study, 89 percent of Black male HICPs say they find care work satisfying. When it comes to feeling appreciated in their roles as caregivers, about three-quarters say they feel respected by their family members (77 percent) or by individuals outside of their family (76 percent).
Despite the satisfaction that unpaid care work brings, for some Black male HICPs, caregiving comes with its own challenges and can, at times, feel like a heavy responsibility. A considerable number of Black men who have cared for a child with special needs or adults find caregiving stressful and experience emotional fatigue in their role. About half (51 percent) find caregiving more stressful than other kinds of work they perform and 48 percent feel burnt out by the unpaid care work they provide.
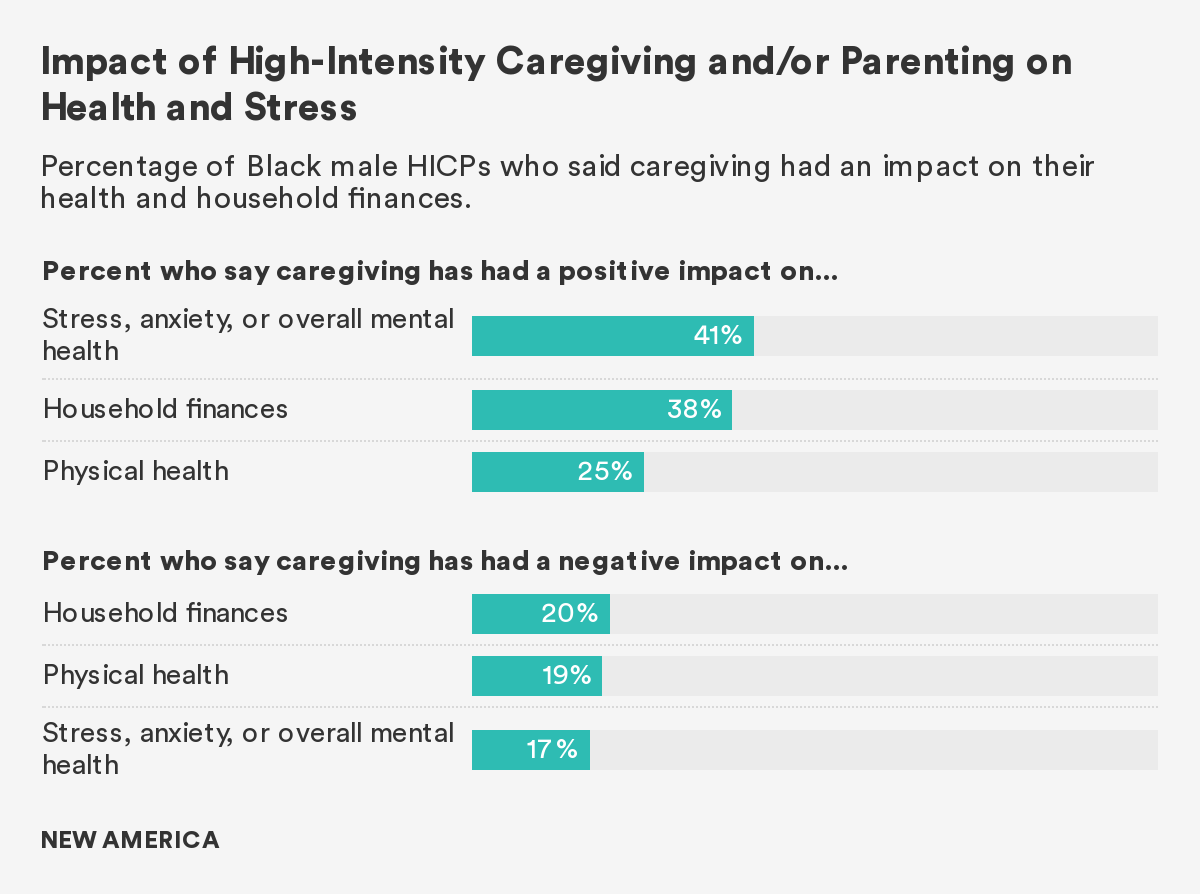
Surprisingly, a larger percentage of Black male HICPs said that caregiving had a positive—rather than a negative—effect on their health and finances. Forty-one percent said that caregiving positively affected their mental health, a quarter credited it with benefiting their physical health, and more than a third (38 percent) noted it had a positive impact on their household finances. These findings are complicated by other studies which examine the health and financial wellbeing of Black adult caregivers and Black individuals relative to that of their white counterparts.
Some research finds that Black caregivers of adults, despite reporting lower levels of stress, carry heavier care burdens.4 According to the National Alliance for Caregiving’s 2020 report, Caregiving in the U.S., on average, Black caregivers report providing more hours of care each week (31.2 hours) than either white (21.2 hours) or Asian American (24.1) caregivers.5 Other studies report that Black caregivers experience higher rates of depression and have lower scores of overall well-being than their white counterparts when they are living with care recipients.6 Research from the National Institute on Minority Health and Health Disparities find that Black individuals have a higher levels of chronic stress and depression in comparison to their white counterparts.7 Furthermore, it has been well documented that Black caregivers do experience the strain of caregiving on their pocketbooks; some cut back on savings or assume debt during their unpaid caregiving career.8
It’s worth noting that respondents in our Men and Care survey self-reported their levels of stress and financial state. Some research on mental health finds that Black individuals report low and high levels of psychological well-being depending on the assessment tool utilized.9 Moreover, researchers find that culture plays an integral role in shaping how people perceive their symptoms, adopt coping mechanisms, and approach treatment.10
Policy Recommendations
Black male HICPs would benefit from sustained investment in financial and supportive services at the federal and state level. Depending on the state they reside in, individuals providing high-intensity care to adults and/or children may receive some form of financial assistance to defray the costs of goods and services related to caregiving or for respite care.11 Respite care allows family caregivers to take a momentary break from supporting care recipients who need help with activities of daily living. The eligibility of a care recipient may indirectly inform whether or not a caregiver can receive financial assistance or compensation for time spent providing care. Apart from programs administered through the Veteran’s Administration which provide caregivers of adults with avenues for support, there currently exists no other widely accessible federal program that provides financial assistance or relief directly to caregivers.
Medicare, public insurance for people 65 years of age and older, does not provide any form of financial compensation for long-term services, like in-home care or adult day centers, which can be most beneficial to care recipients who need assistance with activities of daily living. In 2020, the federal government allocated $185,936,000 to the National Family Caregiver Support Program, which was established in 2000 through the Older Americans Act.12 The National Family Caregiver Support program provides states with funds to administer the program in collaboration with Area Agencies on Aging and local service providers. These regional and local programs then connect caregivers to supportive services (like respite care, caregiver training, and counseling), as well as information and additional assistance.
However, according to a 2016 program evaluation by the Administration for Community Living (ACL), all Area Agencies on Aging in all participating states had at least one waitlist and more than a quarter had multiple.13 A following 2018 report by the ACL concluded that caregivers who were able to access the National Family Caregiver Support program benefited from respite care, training and educational resources, but advocates note that in 2019, only 740,000 people—a mere fraction of the high-intensity caregiver population—had access to the services provided by the National Family Caregiver Support Program.14 The demands for the resources provided through this federal program are high, but historically, its accessibility has been low. Since 2016, there have been calls for increased funding.15
Federal lawmakers should seek additional opportunities and avenues to increase the accessibility of supports and services that promote the health and financial well-being of caregivers. In 2019 and 2020, Congress made progress on the Lifespan Respite Reauthorization Act, extending and revising the Lifespan Respite Care Program, which “supports state lifespan respite care services (i.e. services for family caregivers of children and adults with special needs).”16 The initial version of the legislation passed by the House of Representatives in 2019 allocated $200 million dollars to support coordinated respite services, increase access, and build up the respite care workforce and volunteer corps.17 At the state level, laws like the Caregiver Advise, Record, Enable (CARE) Act, championed by AARP, ensures that family caregivers who provide medical care receive adequate training and information from healthcare professionals when a care recipient is discharged from the hospital; already, 40 states have enacted or are in the process of enacting the law.18
Work-Family Conflict for Black Men who Provide High-Intensity Care to Adults and/or Children with Special Needs
In this study, over half of all employed Black men with unpaid high-intensity caregiving and/or parenting responsibilities find that work demands—more than family responsibilities—very often or sometimes make it difficult for them to spend time with and care for their families.
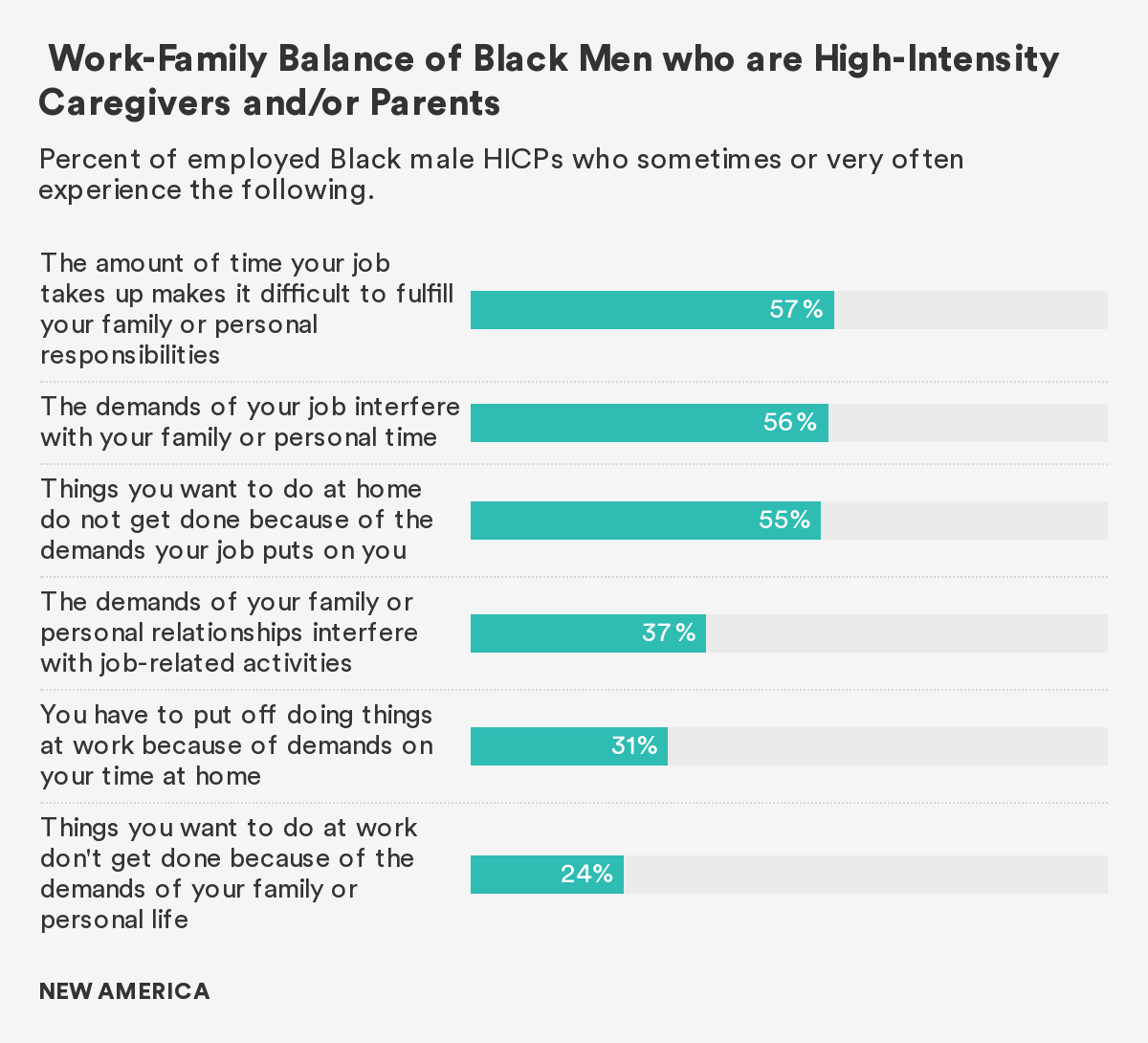
Black male HICPs in our survey point to their jobs, not their families, as the source of work-family conflict. Fifty-six percent of caregivers said that the demands of their jobs very often or sometimes interfered with their family and personal time. When it comes to accomplishing responsibilities at home, 55 percent of caregivers also find that they have to leave certain tasks undone because of the demands of their job. Moreover, 57 percent of caregivers say that the time their jobs take up makes it especially difficult for them to fulfill their family or personal obligations. For Black men, work—more so than family and caregiving responsibilities—is the problematic variable in the work-family balancing equation.
Far fewer Black male HICPs attribute untenable work-family situations to the demands of family life. About one-quarter (24 percent) of caregivers are unable to accomplish certain job-related tasks due to the demands of their family life, 37 percent have to put off doing things at work due to their with familial or personal relationships, and about one-third (31 percent) feel that the demands on their time at home conflicts with what they’d like to accomplish at work.
Policy Recommendations
Black male HICPs would benefit from access to flexible work arrangments with robust caregiver anti-discrimination and anti-retaliation statutes. The Society for Human Resource Management (SHRM) outlines possible flexible work arrangements which may include the following: telework, flextime to begin or end work earlier or later, and use of leave.19 Additional examples of flexible work options include: good part-time work with benefits and the possibility for advancement; the ability to dial up or dial back career progression, depending on caregiving needs and time of life; and stable, predictable schedules for hourly workers that give them more say and control in setting them.
Research demonstrates that access to flexible work arrangements can help reduce work-life conflict, increase employee engagement, and decrease work-related stress.20 Policies aimed at increasing workplace flexibility already exist. For example, in the United Kingdom, all workers have the right to request flexible work arrangements. In the City of San Francisco, caregivers can benefit from the San Francisco Family Friendly Workplace Ordinance, which permits workers to request flexible work arrangements or more predictable scheduling, allowing to care for a family member or child as needed.21
Barriers to Leave for Black Men who are High-Intensity Caregivers and/or Parents
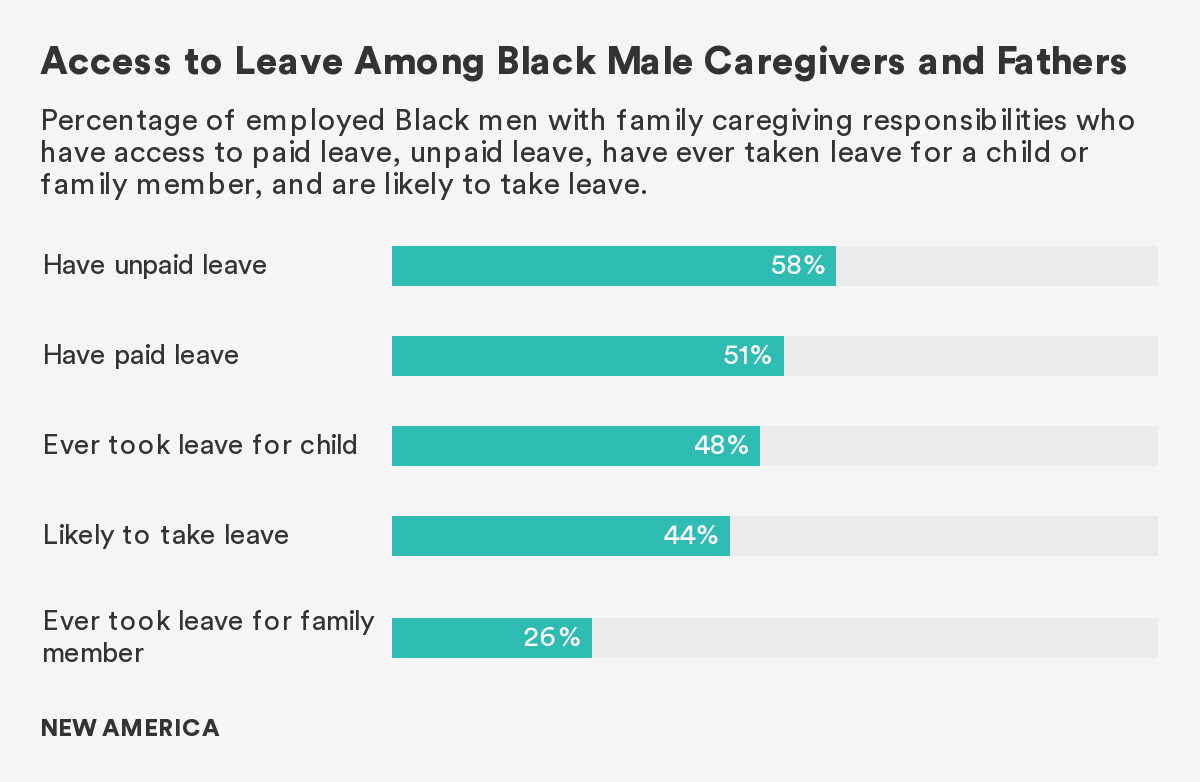
More Black men providing high-intensity care to adults and/or children with special needs have access to unpaid leave than to paid leave.
In 2019, the Better Life Lab published Lifting the Barriers to Paid Family and Medical Leave, which found that men anticipate needing to take time off from work for caregiving, and that a universal paid leave policy would best support them in their various roles.22 The report also highlighted the barriers that make it harder for men to access and take leave, among them an inability to afford unpaid or partially paid leave and workplace cultures (and practices) that disincentivize men from using it. In our survey, Black men find themselves in a similar predicament to men overall; they want to spend more time providing care, but face a number of barriers that prevent them from doing so.
Among employed Black men who are high-intensity caregivers and/or parents, a little more than half (51 percent) say they have access to some form of paid leave and 58 percent have unpaid leave. Only 46 percent say they have ever taken any kind of leave (sick time, vacation time, paid family-medical leave, or any other kind of leave) for more than a day or two following the birth or adoption of a child. Just 26 percent have ever taken leave for more than a day or two to care for a family member with a serious illness, or a disability, or who needs extra help as they get older. These findings show that even when Black men have access to leave, a smaller percentage actually use it. Accoring to our survey, forty-four percent of Black male HICPs anticipate needing to take time off sometime in the future; however, their decision and capacity to take leave will depend in large part on their ability to afford the costs associated with it.
A majority of Black men who are high-intensity caregivers and/or parents think that the costs associated with taking leave prevents men from using it. More than one-third worry that workplace penalties disincentivize men from taking time off from work for caregiving.
Many caregivers struggle to afford taking time off from work to provide care to a loved one, and Black men are no exception. In the United States, the national leave policy—the Family and Medical Leave Act (FMLA)—only provides 56 percent of the workforce with twelve weeks of job-protected unpaid leave.23 According to the Bureau of Labor Statistics, just 20 percent of civilian workers have dedicated paid family and medical leave through their employer to care for a new child or an ill loved one—and those who are covered by an employer's policy tend to earn higher wages and work in professional, white-collar jobs.24
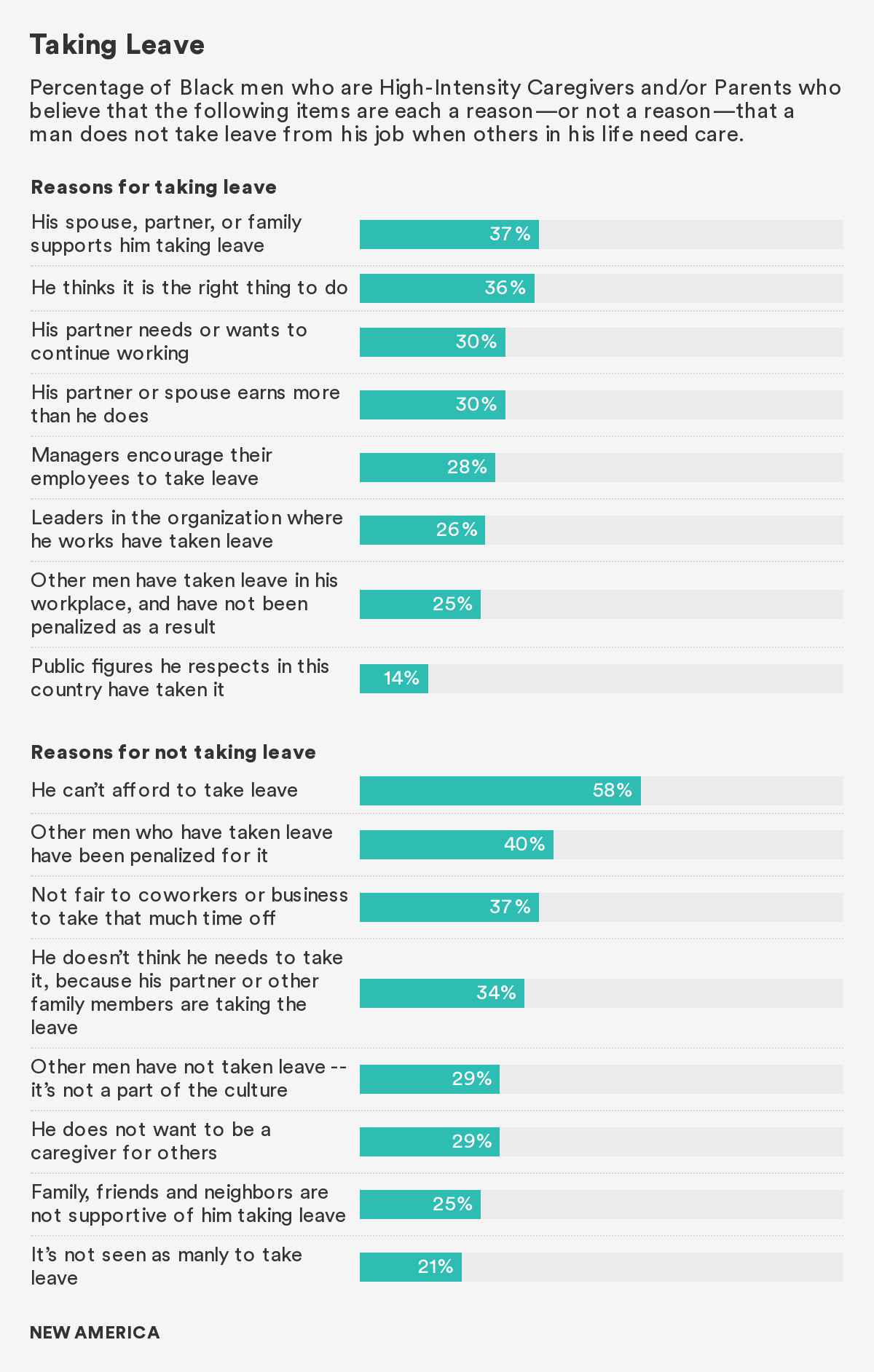
Fifty-eight percent of all Black men who provide high-intensity care to an adult or child with special needs think that a major disincentive to men’s use of leave is an inability to cover the costs associated with taking time off from work. In addition to affordability, there are a number of other reasons why men do not take advantage of leave (paid or unpaid) even if they have access to it.
Family expectations play a role in influencing men’s decisions around taking time off to provide care. Thirty-four percent do not think they need to take caregiving leave because their partner/spouse is taking it, 29 percent do not wish to provide care, and one-quarter face discouragement from those closest to them—family, friends, and neighbors. Of course, apart from personal motivations and perceived expectations of family and friends, structural barriers, namely workplace expectations and culture, prevent the use of leave amongst Black male HICPs.25
Fears and concerns about work inform whether or not men choose to take leave.
Workplace cultures in the United States by and large make it hard for employees to manage their work and care obligations. Though women, and particularly mothers, suffer most, men also face barriers to care and spending quality time with their families.
In our survey, 40 percent of Black male HICPs say men may not take leave if they fear being penalized at work. More than one-third (37 percent) think that men will not take time off if they think that their absence will burden their coworkers. Twenty-nine percent of Black male HICPs think that men, observant of their surroundings and the behaviors of their peers, will not take leave if they feel that it’s not part of the culture and don’t see other men using the benefit.
Despite worries that the inflexibility of workplace structures, cultures, and coworkers will disincentivize men from being the caregivers they’d like to be, more than a quarter of Black male HICPs think that certain characteristics in the workplace could actually encourage men to take time off to give care: men will take leave if there are no penalties (25 percent), if leaders in the organization take leave (26 percent), and if managers actively encourage workers to use the benefit (28 percent). Our findings corroborate years of research that demonstrates that workplace culture, expectations, and policies have the power to either disincentivize or encourage leave use amongst men.26
Policy Recommendations
Black male HICPs would benefit from a combination of federal, state, and workplace policies that provide them access to paid leave and promote their use of it. The existing national family leave law—FMLA—is unpaid and its eligibility requirements exclude millions of workers in the United States. Moreover, it does not protect a caregiver's right to take time off to tend to a family member who is not a spouse, a child, or a parent. Black men providing high-intensity care to adults and/or children with special needs, like all caregivers, may need to care for a sibling, a grandparent, an aunt, a cousin, or a friend; but these caregiving relationships are not accounted for in the FMLA. Additionally, as this report has shown, the existing national paid leave policy may not support Black male HICPs who cite affordability as one of the key reasons why men don’t take leave.
Forty-four percent of Black male HICPs anticipate needing to take time off. A robust, national paid family leave program would likely help ensure they have the financial security to do so. Congress passed the Families First Coronavirus Response Act of 2020 (FFCRA), as part of an emergency relief package. The act instituted the first, national, paid leave program in the U.S. Though temporary through the end of 2020—available only to those whose children were home because of school and childcare shutdowns—and largely inaccessible to millions due to generous exemptions for large and small businesses, it served as a first step toward a permanent, more robust policy.
A permanent paid leave policy that would best help Black men with high-intensity care responsibilities would not only be paid, but it would also have adequate wage replacement. States that have adopted paid leave programs have used a social insurance model, funded through small payroll deductions to provide benefits to workers who need to take time off to care for a child, seriously ill or disabled loved one, or for their own serious health issues. The states utilize different methods for compensating caregivers. The two most common are progressive/sliding scale wage replacements that provide a larger percentage of wages for low-income workers (up to 90 percent in Washington state) and fixed percentages.
Research demonstrates that low-wage replacements disincentivize the taking of leave among men. It also particularly impacts workers in industries with lower wages, which are disproportionately occupied by people of color who have less access to wealth and the resources needed to financially weather sudden emergencies. To be truly effective, especially for men and Black men, a national paid leave program would need to not only establish adequate wage-replacements, but also support policies and practices that actively promote the use of leave among all workers with caregiving needs. A robust policy must include job-protections so that caregivers can return to the same or a similar position after taking leave, and improved outreach to and educational resources for both workers and employers, to increase awareness and full utilization of the program.
Having access to paid leave isn’t enough; Black men providing high-intensity care to adults and/or children with special needs must feel supported in their decision to use paid leave. Forty percent of Black male HICPs in this study said that workplace penalties would deter men from taking leave. Workplaces can create environments that encourage rather than penalize leave taking among men employees. Using gender-inclusive language in employer leave policies could disrupt the cultural notion that men don’t take leave; it could begin to normalize the reality that they have care responsibilities that influence their performance and presence in the workplace.27 Moreover, Black male HICPS should see role models of men and leaders use the benefit, thereby making it “safe” for others to do so without undue fear or concern about retaliation. Modeling the use of leave at the leadership and managerial level could positively influence men’s decisions to take leave; research demonstrates that when leaders in the workplace model healthy behaviors or take advantage of work benefits, they create a culture that influences employees’ decisions to do the same.28
Policymakers and workplace leaders can craft, adopt, and implement robust, family-supportive policies that protect Black men's rights to give care and promote equitable access to resources that ensure they have opportunities to do so without the fear of losing pay or even their jobs. Introduced by the Senate in June 2020, the Protecting Family Caregivers from Discrimination Act is one example of proposed legisaltion that seeks to encourage family supportive workplaces.29
Increasing access to paid leave is a form of economic and racial justice. A national, permanent paid leave policy with robust job-protections and adequate wage-replacements would especially benefit Black male HICPs because it would lessen the compounding impact of current economic barriers to caregiving. A report from the Economic Policy Institute (EPI) outlines the various economic racial disparities that disadvantage Black individuals, particularly in the labor force.30 Black workers, both men and women, face a higher likelihood of unemployment in comparison to their white counterparts, regardless of their level of education.31
The Federal Reserve Board reports that as of July 2020, Black workers were more likely than their white counterparts to report a recent layoff. On average, Black workers receive less pay and face a growing wage gap.32 Moreover, they have less access to benefits, like paid sick days and flexible work arrangements. According to EPI, the median household incomes for Black families are 70 percent lower than that of white households. In 2016, the average Black family had $17,600 in wealth compared to white families’ average of $171,000. Lower wages, hence less income, contributes to the racial wealth gap.33
Such disparate economic outcomes have their roots in a long history of policies and practices that fueled employment discrimination, inequitable access to education, labor market segregation, and unequal access to wealth in the form of housing, savings, and other assets. Policies like FMLA do little to decrease the economic challenges disproportionately experienced by Black workers and families—if anything, they exacerbate them, especially if an emergency arises. Research finds that Black families have less access to savings, which serves as a financial safety net and are more likely to accumulate medical debt.34 For Black families, the median costs associated with taking unpaid leave for 12 weeks would amount to more than $8,077.35 Black men who provide high-intensity care—and their families—are among those who would stand to gain the most from a national paid leave policy.
Policies and programs would prove most equitable and impactful if crafted with an understanding of the various economic barriers sustained by systemic racism that inform how Black male caregivers navigate their lives and undoubtedly shape their caregiving experiences.
Comparing Black and White Men who are High-Intensity Caregivers and/or Parents
In our survey, Black and white men providing high-intensity care to adults and/or children with special needs are more similar than different from one another in how they value caregiving, what tasks they perform, and the barriers they face as caregivers. The policies and programs that would benefit Black male HICPs would likely benefit other caregiving men as well.
Valuing Care
As it pertains to attitudes about care, the similarities between Black and white men who are high-intensity caregivers and/or parents is striking. An overwhelming majority of both groups value caregiving, and on all six survey questions asked about this topic, there were no significant differences between men of the two races. For example, more than 70 percent of men in both groups say they are proud to talk with their family and friends about the role they play in caring for their family, and believe that being an engaged father is an important part of being a man.
When it comes to gender roles in the family, a majority of Black and white male HICPs (more than 80 percent of both groups) agree that men and women should divide caregiving responsibilities equally at home. While a majority of Black and white men espouse positive views of caregiving, a smaller percentage across both racial groups, actually observe men in their communities performing more care work than women. More than half of Black and white male HICPs say they live in a community where most men do less care work. Regardless of what they observe, a majority of both groups (more than 80 percent) believe that care work performed in the home is meaningful to society.
High-Intensity Caregiving and/or Parenting
Out of the eight physical and instrumental daily living care tasks our survey asked about, there was only one significant difference between Black and white men who have ever provided care to adults or children with special needs: More white men (78 percent) than Black men (61 percent) report shopping for groceries.
Apart from that, similar percentages of both groups remind adult care recipients to take their medication, handle care recipients’ bills, cook for them, provide household maintenance and cleaning, and manage their appointments. Across both groups, more than a third assist with bathing.
The most noteworthy differences between Black and white men pertain to nursing-level medical tasks. Twenty-seven percent of Black male HICPs perform or administer injections, 21 percent care for an IV or port, and 18 percent prepare or insert tubes for feeding or catheters. In contrast, 12 percent of white male HICPs administer injections, 8 percent care for an IV or port, and 7 percent insert or prepare feeding or catheter tubes. Also, more Black men (53 percent) than white men (37 percent) administer medications to care recipients who require them. Despite these differences, at least one-quarter of both groups perform other medical care tasks like checking blood pressure or blood glucose and changing bandages or caring for wounds.
Leave and Work-Family Balance
Unfortunately, Black and white men providing high-intensity care to adults and/or children with special needs are also similar in that they both face barriers that limit their ability to give care. On the issue of work-family balance described in the second part of this report, white male HICPs were more likely than Black men to say that the demands of their jobs prevent them from performing tasks at home (74 percent and 55 percent, respectively). Nevertheless, the pattern was the same for Black and white men who provide high-intensity care. In general, Black and white male HICPs were both more likely to indicate that their work, more so than their family responsibilities, caused conflict between the personal and professional spheres of their lives.
In addition to workplace demands, accessibility and affordability of leave pose another barrier to men’s abilities to provide care as high-intensity caregivers and/or parents. Only about half of male HICPs in both racial groups have access to paid leave—fewer Black men (58 percent) than white men (67 percent) have access to unpaid leave. About half have ever taken leave to care for a child, and at least one-quarter have taken leave to care for a family member. More than one-third of caregivers in both groups anticipate needing to take leave in the future. However, more than half of Black and white male HICPs (white men more than their Black counterparts), think that an inability to afford leave would be a disincentive from doing so.
For Black and white men fulfilling the role of high-intensity caregiver and/or parent, the decision to take leave also depends upon workplace culture and expectations. At least 40 percent of both groups worry that the potential for penalties will deter men from taking leave. Still, more than one-quarter of men in both groups are optimistic that men will take leave if managers encourage the practice, and one-quarter think that men will take leave if they see other men in the workplace using the benefit. Generally, when thinking about whether or not to take time off from work to provide care, men want reassurance—rather than the threat of punishment—from their colleagues and supervisors.
These findings demonstrate that caregiving is a universal experience and that the policies that would support Black men providing high-intensity care would likely benefit other men as well. Moreover, these results reinforce the reality that the caregiving challenges that Black men experience are not due to personal decisions nor behaviors–rather, they are due to structural problems that require structural responses.
Citations
- Physical activities of daily living are described as the tasks essential to maintaining one’s personal hygiene, like bathing, grooming, dressing, eating, and ambulating. Instrumental activities of daily living refers to tasks essential to navigating personal affairs like paying bills, managing medication, housekeeping, etc. In our survey question, we used different language and categorized these caregiving tasks into two categories: either hands-off, or hands-on. Refer to graph for more details. (Peter F. Edemekong et al., “Activities of Daily Living,” in StatPearls (Treasure Island (FL): StatPearls Publishing, 2020), source.)
- National Alliance for Caregiving and AARP, Caregiving in the U.S. 2020, source.
- Susan C. Reinhard, Heather M. Young, Carol Levine, and Kathleen Kelly, Rita B. Choula, Jean Accius, Home Alone Revisited: Family Caregivers Providing Complex Care, (Washington, D.C.: Founders of the Home Alone Alliance, April 2019), source.
- Family Caregiver Alliance, “Caregiver Statistics: Demographics,” April 17, 2019, source.
- National Alliance for Caregiving and AARP, Caregiving in the U.S. 2020, source.
- Ilene C. Siegler et al., “Caregiving, Residence, Race, and Depressive Symptoms,” Aging & Mental Health 14, no. 7 (September 2010): 771–78, source.
- National Institutes of Health (NIH), “African Americans and Latinos Are More Likely to Be at Risk for Depression than Whites,” May 24, 2018, source.
- National Alliance for Caregiving, “The ‘Typical’ African American Caregiver,” Fact sheet, May 2020, source.
- David R. Williams, “Stress and the Mental Health of Populations of Color:Advancing Our Understanding of Race-related Stressors,” Journal of Health and Social Behavior 59, no. 4 (2018): 466–485, source">source.
- Office of the Surgeon General et al., "Chapter 2 Culture Counts: The Influence of Culture and Society on Mental Health," Mental Health: Culture, Race, and Ethnicity: A Supplement to Mental Health: A Report of the Surgeon General, (Washington, D.C.: Office of the Surgeon General), August 2001, source">source.
- Family Caregiver Alliance, "Frequently Asked Questions," last accessed December 17, 2020, source; ARCA National Respite Newtork and Resource Center, "Fact Sheet: Nine Steps to Respite Care for Family Caregivers of Children and Adults with Intellectual and Developmental Disabilities," March 2018, source.
- Administration for Community Living, “Fiscal Year 2021 – Justification of Estimates for Appropriations Committees” (U.S. Department of Health and Human, June 2020): 103, source; “National Family Caregiver Support Program,” ACL Administration for Community Living, November 12, 2019, source; “Older Americans Act,” ACL Administration for Community Living, July 21, 2020, source.
- The Lewin Group, Inc, Process Evaluation of the Older Americans Act Title III-E National Family Caregiver Support Program: Final Report (Washington, D.C.: The Administration for Community Living, March 2016), source.
- Cecilia Avison et al., Outcome Evaluation of the National Family Caregiver Support Program, (Washington, D.C.: Administration for Community Living, December 2018), source; Lynn Friss Feinberg, “Strengthening the National Family Caregiver Support Program: The Time Has Come,” AARP Blog, March 11, 2019, source.
- National Academies of Sciences, Engineering, and Medicine, Families Caring for an Aging America, (Washington, DC: The National Academies Press, 2016), source.
- James R. Langevin, “Actions – H.R.2035 – 116th Congress (2019-2020): Lifespan Respite Care Reauthorization Act of 2019,” webpage, July 25, 2019, source.
- Policy Division of the ARCH National Respite Network, “Reauthorize Lifespan Respite,” last updated December 10, 2020, source.
- AARP, “New State Law to Help Family Caregivers,” accessed December 17, 2020, source.
- Ellen Ernst Kossek et al., “Leveraging Workplace Flexibility for Engagement and Productivity,” Effective Practice Guidelines Series (Alexandria, VA: Society for Human Resource Management, 2014), source.
- Ellen Ernst Kossek et al., “Leveraging Workplace Flexibility for Engagement and Productivity,” source.
- Gov.UK, “Flexible Working,” source, accessed December 17, 2020.; David Chiu, “San Francisco Family Friendly Workplace Ordinance Legislative Fact Sheet,” San Francisco Board of Supervisors, accessed December 17, 2020, source.
- Amanda Lenhart, Haley Swenson, and Brigid Schulte, “Lifting the Barriers to Paid Family and Medical Leave for Men in the United States” (Washington, D.C.: New America, December 4, 2019), source.
- Vicki Shabo, “Explainer: Paid and Unpaid Leave Policies in the U.S.,” New America, December 14, 2020, source.
- Eugene Scalia and William W. Beach, “National Compensation Survey: Employee Benefits in the United States” (Washington, D.C.: U.S. Bureau of Labor Statistics, March 2020), source; Trish Stroman et al., “Why Paid Family Leave Is Good Business” (Boston: Boston Consulting Group, February 2017), source.
- Deloitte, “Deloitte Survey: Less Than Half Of People Surveyed Feel Their Organization Helps Men Feel Comfortable Taking Parental Leave,” Cision PR NewsWire, July 15, 2016, source.
- Amanda Lenhart, Haley Swenson, and Brigid Schulte, “Lifting the Barriers to Paid Family and Medical Leave for Men in the United States,” source; “Working Dads across the United States Want Better Paid Family Leave.,” PL+US, June 16, 2019, source.
- AEI-Brookings Working Group and on Paid Family Leave, “The AEI-Brookings Working Group Report on Paid Family and Medical Leave” (Washington, D.C.: American Enterprise Institute and Brookings Institution, September 2018), source.
- Caroline Kranabetter and Cornelia Niessen, “Managers as Role Models for Health: Moderators of the Relationship of Transformational Leadership with Employee Exhaustion and Cynicism,” Journal of Occupational Health Psychology 22, no. 4 (2017): 492–502, source.
- Cory A. Booker, “Text – S.3878 – 116th Congress (2019-2020): Protecting Family Caregivers from Discrimination Act of 2020,” webpage, June 3, 2020, 2019/2020, source.
- Elise Gould and Valerie Wilson, “Black Workers Face Two of the Most Lethal Preexisting Conditions for Coronavirus—Racism and Economic Inequality,” (Washington, D.C.: Economic Policy Institute, June 1, 2020,) source.
- Valerie Wilson, “Racism and the Economy: Focus on Employment,” Working Economics Blog, Economic Policy Institute, November 21, 2020, source.
- Consumer and Community Research Section of the Federal Reserve Board’s Division of Consumer and, and Community Affairs (DCCA), “Update on the Economic Well-Being of U.S. Households: July 2020 Results,” (Washington, D.C.: Federal Reserve Board, September 2020), source.
- Aria Florant et al., “The Case for Accelerating Financial Inclusion in Black Communities,” McKinsey & Company, February 25, 2020, source.
- Angela Hanks, Danyelle Solomon, and Christian E. Weller, “Systematic Inequality: How America’s Structural Racism Helped Create the Black-White Wealth Gap” (Washington, D.C.: Center for American Progress, February 21, 2018), source.
- Diversity Data Kids, “Making Leave Affordable,” February 2018, source.