
Table of Contents
Distances to Travel to Hospital-Based Health Care
Rural workers’ lower levels of access to paid leave benefits, greater and growing caregiving needs, and overall worse health relative to metropolitan areas—combined with greater financial insecurity and lower incomes—means that long distances to health care may pose significant challenges for rural workers who need health services for themselves or a loved one.
Our work builds on literature focused on rural hospital closures and distances to particular types of health services, for example breast cancer and lung cancer imaging. We add to this research for particular populations, with a lens on the intersections between lack of access to paid leave and long distances to receive hospital-based health care services and treatments.1 We specifically examined hospital-based obstetric care, neonatal intensive care units (NICUs) and other neonatal care, pediatric care, cardiac care, and cancer screening and treatment services, comparing mileage-based distances from rural and urban census tracts for each. We also analyzed distances to hospital facilities for rural census tracts with persistent poverty, rural census tracts with high concentrations of Black residents and rural census tracts with high concentrations of Hispanic/Latine residents. Finally, we completed the same analysis for Skilled Nursing Facilities. 2
It is important to note that our analyses reflect the availability of hospital-based services, but some types of services (such as mammography, colonoscopies, and other cancer screenings) are frequently available in outpatient settings and so access may be greater than these analyses would suggest, though people may sometimes require hospital-based care. For other services that nearly always occur in a hospital (neonatal care and neonatal intensive care units, for example), this limitation is less of a concern. It is also important to note that mileage-based distances may understate the difficulty of travel on rural roads in certain areas of the country; for example, in Appalachia, windy roads and poor road quality—especially in bad weather—may make traveling even short distances quite slow and onerous.
We find that people in rural census tracts must travel much further distances than people in urban areas to access hospital-based health care services: often three-to-four times as many miles on average and, for people in remote rural areas, much further than that. We find that many of the closest rural census tracts to health care services are further away from hospital-based health care services than the most distant urban census tracts are to the same kind of health care service.
Our analysis shows that Hispanic/Latine residents in rural communities are the worst off—they have further distances to travel than any other group and, as discussed in the previous section, they have less access to paid sick time and to paid family and medical leave. Census tracts with concentrations of Black residents are slightly closer to the hospital based health care services we examined, likely because a smaller share of Black residents than Latine residents and rural residents overall live in isolated rural census tracts—but health disparities and risk factors (for example, black maternal mortality) make quick access to care an important health imperative, and even shorter distances for this population are still quite significant. Distances for Hispanic/Latine residents and Black residents are also a function of geography: People in rural areas of the West, where Latine populations are concentrated, have further to travel than people in the South, where many Black residents are concentrated.
We find that rural areas with persistent poverty are slightly further than other rural census tracts from hospital-based obstetrics care and cancer screening and moderately further from cancer treatment. Even where distances are similar for all rural areas and areas with persistent poverty, the effects of that travel distance may be greater for low-income households whose workers are far less likely to have access to paid sick time or paid leave.
A. Obstetrics & Neonatal Care
Because maternal health and mother’s labor force participation are key issues for both the health and economic well-being of their children and families—and because pregnancy and parental leave is associated with better outcomes—we look at the distances to hospital-based obstetric care and neonatal units.
Rural women are less likely to have paid leave they can use to recover from childbirth and care for a new child than other women—and the barriers they face to seek care due in part to longer distances are greater. For Black women, who have higher maternal mortality rates and face well-documented bias in the health care system, the ability to get to a high-quality hospital quickly may be a matter of life and death. Moreover, every state in which abortion access is severely limited or has been eliminated entirely has a 20 percent or greater share of rural residents.3 In these states, lack of access to abortion care, plus long distances to hospital-based obstetrics care for births that may not be by choice, create one more hurdle to mental and physical health for birthing people—potentially compounded by lack of paid leave.
1. Obstetrics Care
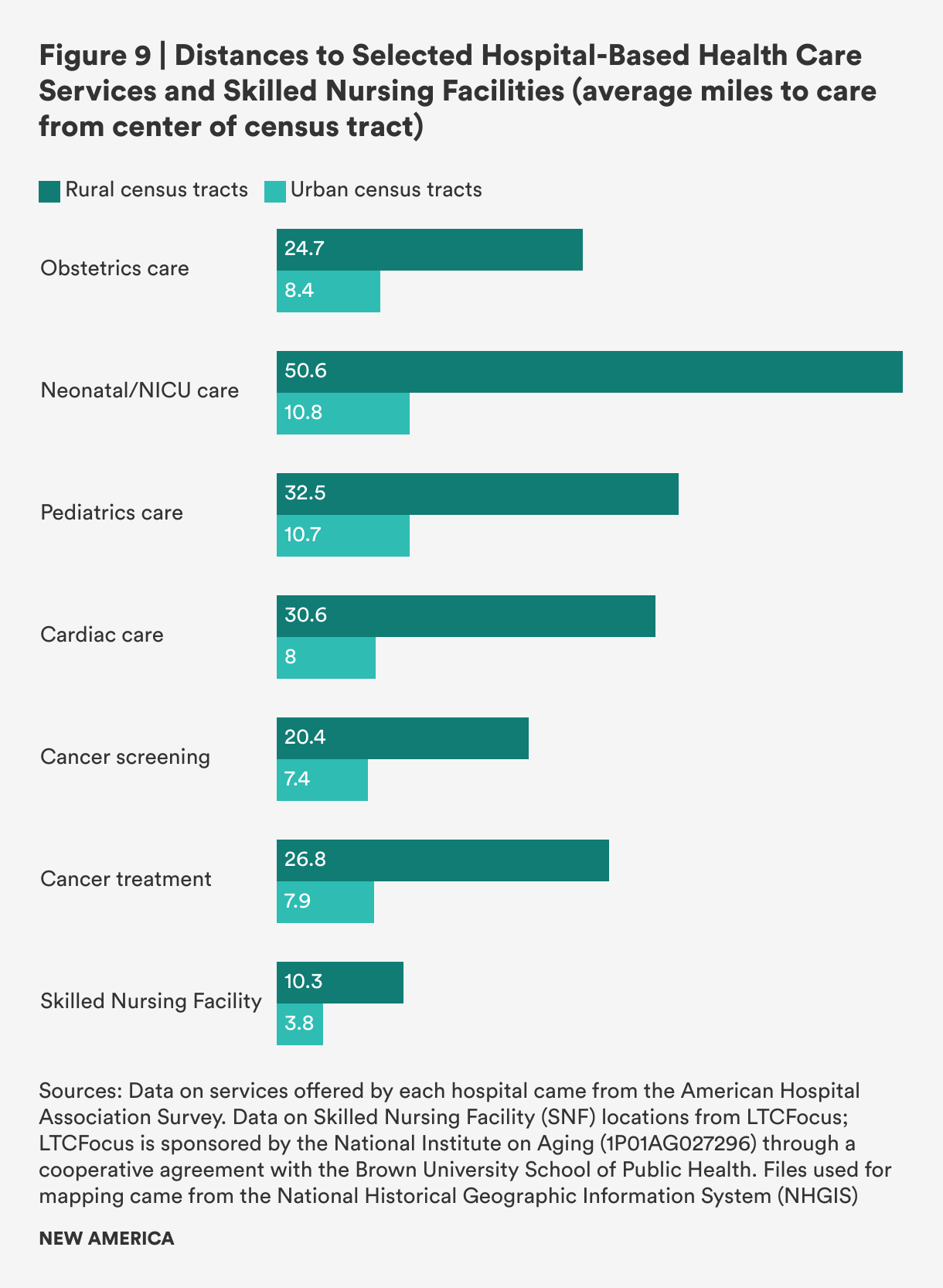
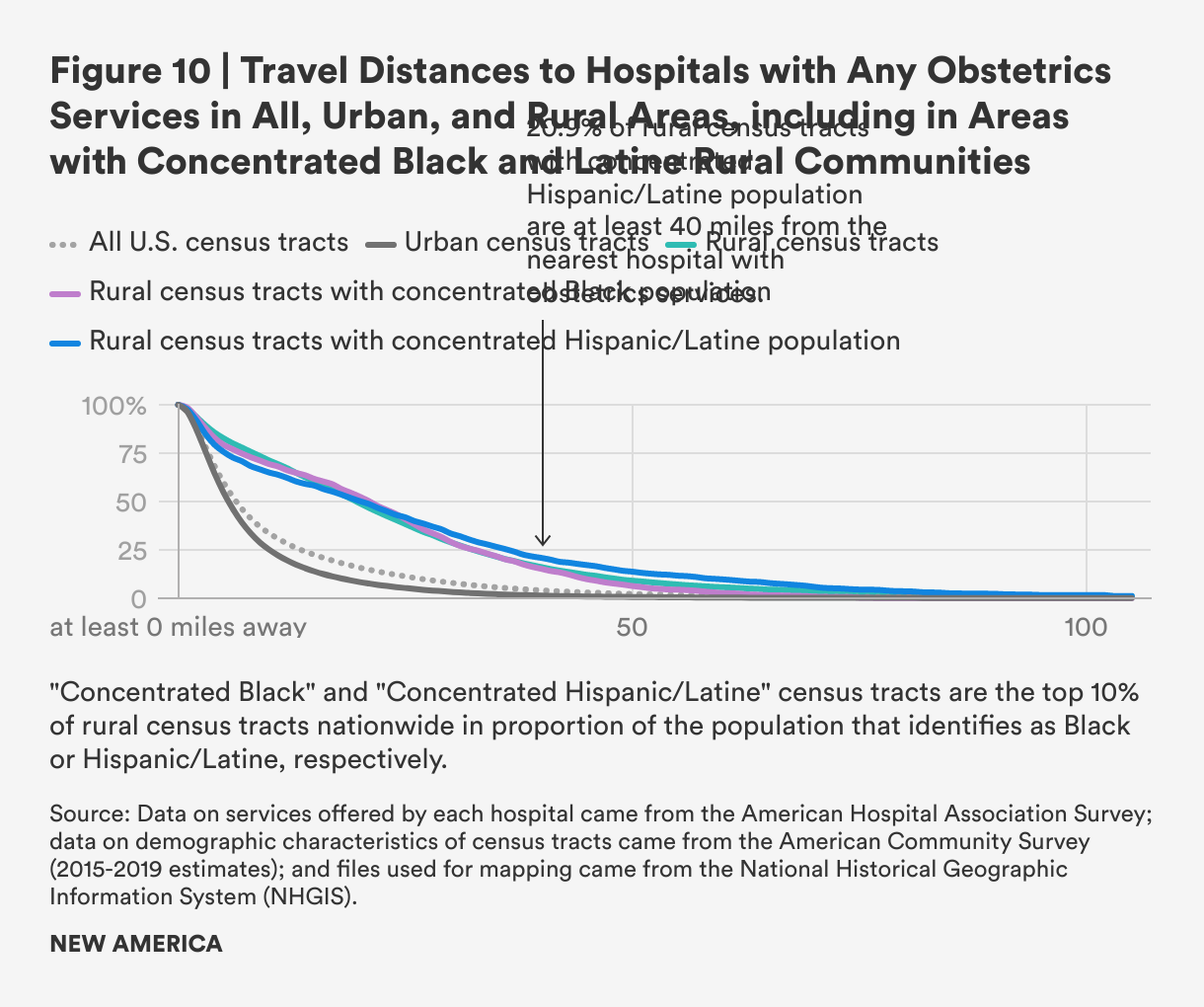
Our analysis shows that the mean travel distance to a hospital providing any obstetrics services is nearly three times further for rural census tracts than for urban ones: 24.7 miles for rural census tracts, compared with 8.4 miles for urban census tracts. Distances to more advanced obstetrics services are likely even more limited and distances even longer for rural residents, but too few hospitals provide information on the level of obstetric care they provided to be more precise.
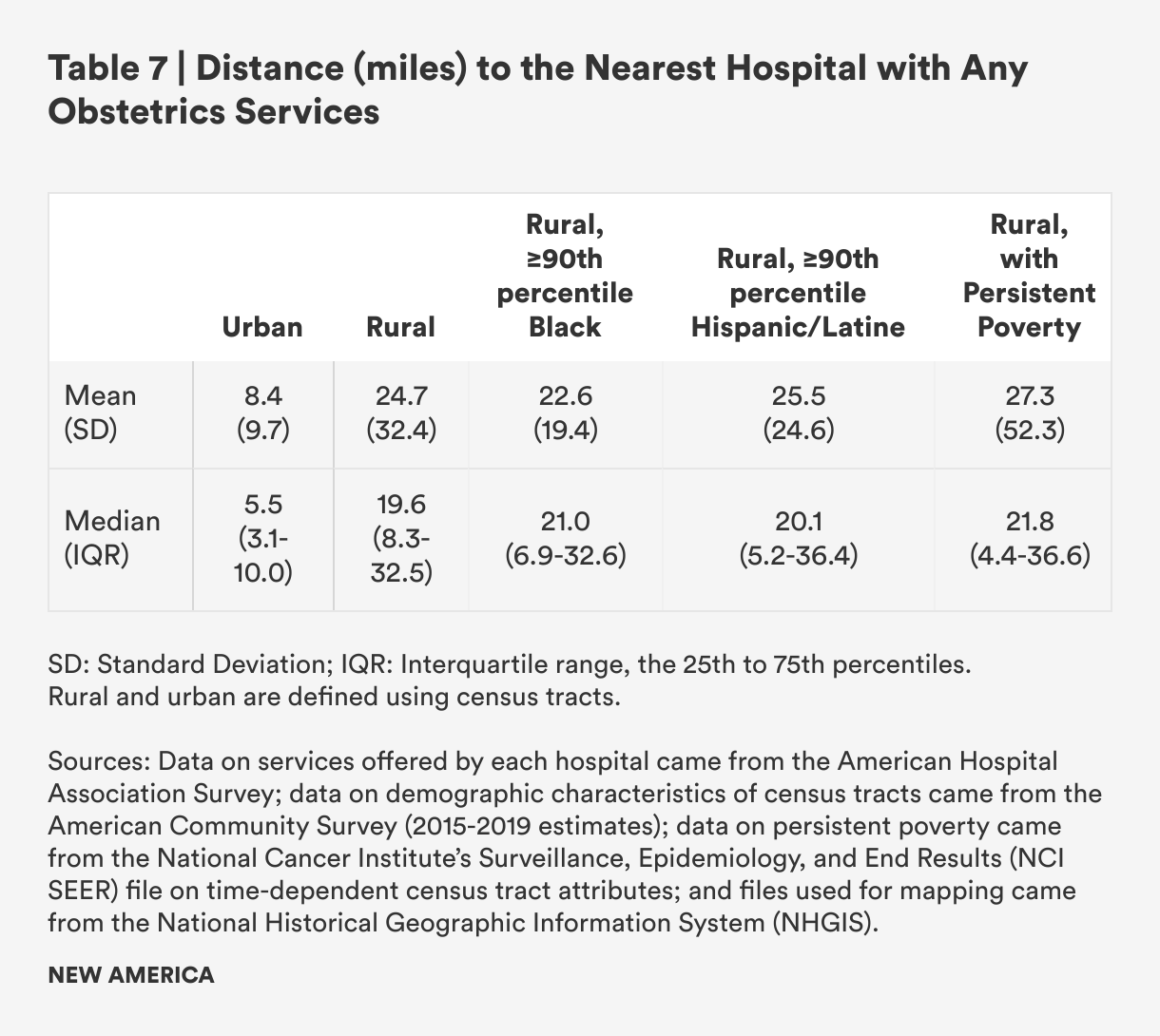
Among rural census tracts, we examined differences in mean travel distance to hospital-based obstetrics care between rural census tracts with persistent poverty compared to those without persistent poverty, those with high concentrations of Black residents compared to those without, and high concentrations of Latine/Hispanic residents compared to those without. We did not find significant differences in travel distances among these subgroups, yet the economic and health effects of long distances to travel to health care may be more pronounced for these communities given lower income, less access to wealth, and—for people in poverty and Hispanic/Latine people—less access to paid leave.
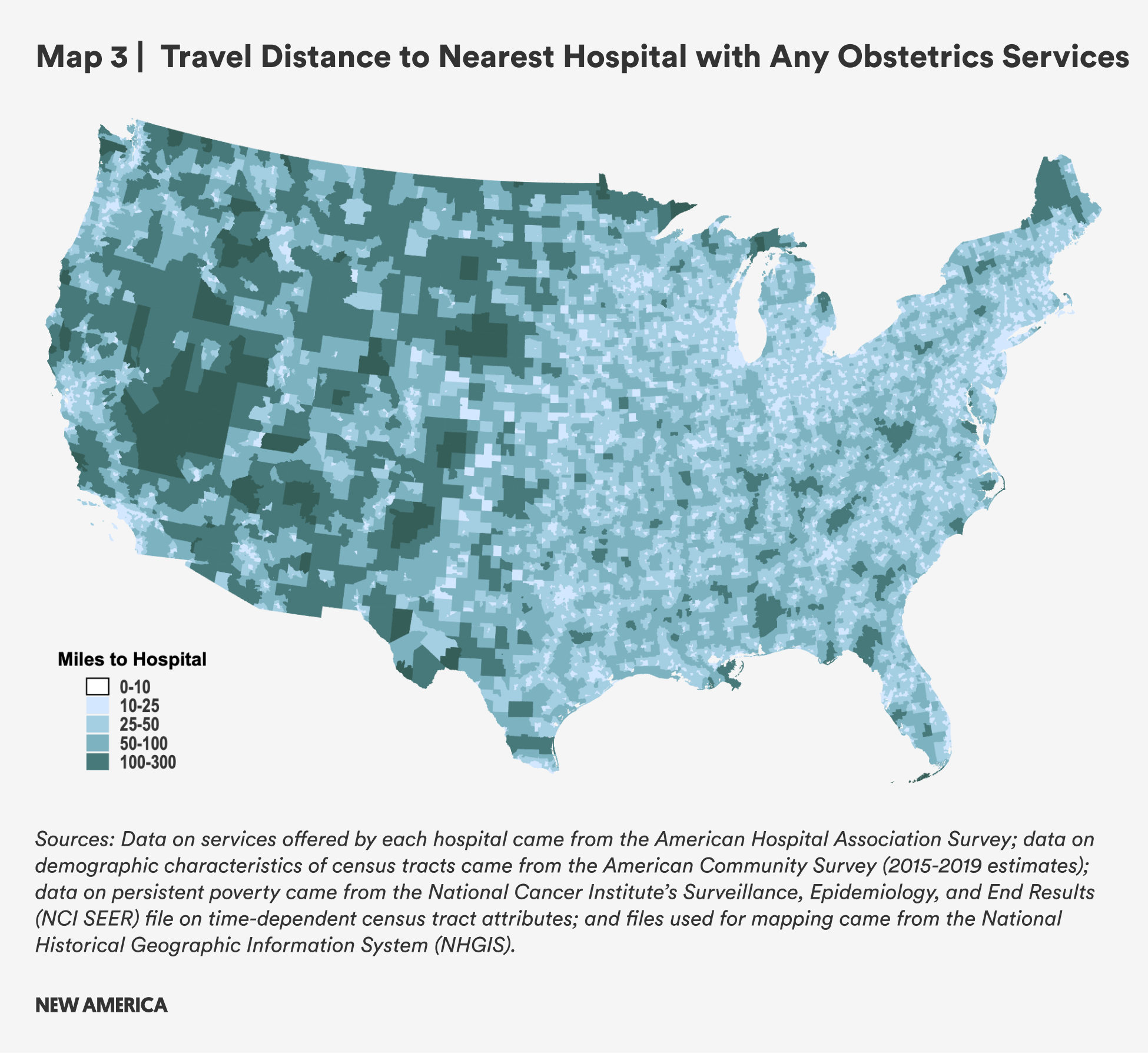
There is significant geographic variation in travel distance. Rural areas in the west experience the highest travel burden, with many of those census tracts more than 100 miles away from the nearest hospital with obstetrics services. In the eastern half of the country, distances are shorter on average, though parts of northern Maine, Michigan, and Minnesota and other spots farther South still face significant travel burdens of more than 50 miles.
2. Neonatal Care
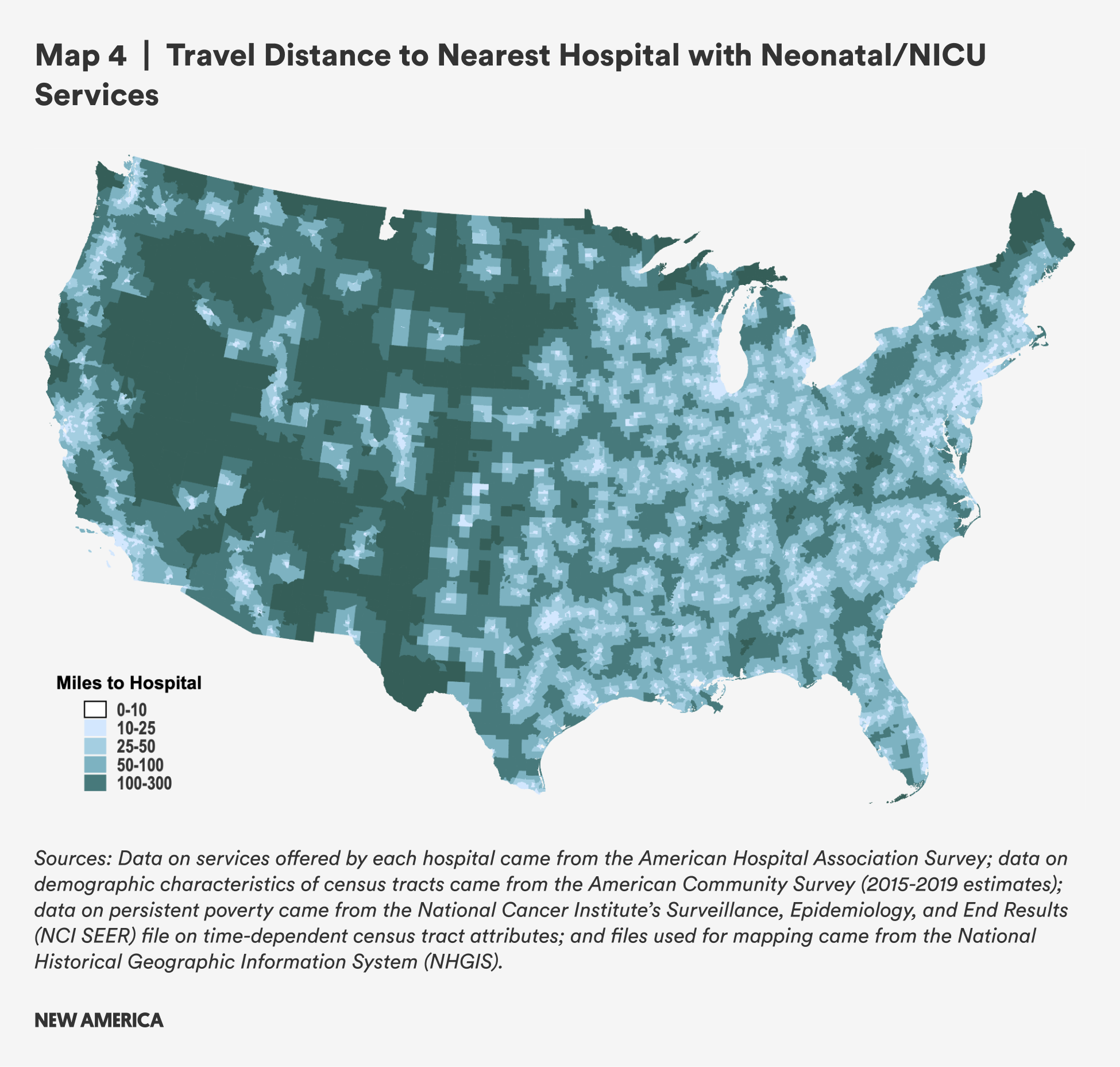
Access to neonatal care and neonatal intensive care units (NICUs) is rarer than obstetrics care, with fewer hospitals reporting that they offer neonatal care or NICUs. The average distance to a hospital with neonatal services in rural areas is nearly five times greater for rural residents than urban residents: 50.6 miles, compared with 10.8 in urban areas. This has implications: one study of dyads composed of mothers and preterm infants which looked at travel times rather than distances is illustrative—mothers who had to travel more than 30 minutes to get to a NICU spent fewer days per week visiting their hospitalized preterm babies.4 For parents whose children must remain in the NICU for periods of days, weeks or months, long distances and long travel times may force impossible choices between work and spending time with and caring for a baby in the NICU.

While there were less significant differences in distances to hospital NICUs and neonatal care between rural tracts with persistent poverty and those without, there were differences by demographics. Rural tracts with higher proportions of Black residents have considerably shorter travel distances on average, while those with high Hispanic/Latine populations have longer travel distances on average.

These findings likely reflect the heterogeneity of rural populations across the country. Rural areas with the largest proportion of Black residents are concentrated in the South, while there are more Hispanic/Latine people in the rural West, where travel burden is greater. As with obstetrics services, many census tracts in the rural West are more than 100 miles aways from the nearest hospital with neonatal services, with only a few areas on the east coast having similar distances.
B. Pediatric Care
Access to care for children with serious health issues is essential. Hospitalized children recover more quickly and with fewer complications if a parent is able to be with them.5 Distances to care can be a barrier for working parents, and lack of access to paid leave creates even more strain on working parents. While all hospitals may provide care to children who require it, these results show the distance to hospitals that specifically report providing pediatric health care, are a pediatric hospital, or who have a pediatric ICU.
Table 9 shows that the mean distance from a rural census tract to a hospital that provides pediatric health services is three times further than in urban census tracts: 32.5 miles compared with 10.7 miles. Median distances are nearly four times greater for rural versus urban census tracts. Distances are not substantively different in rural areas with persistent poverty compared to all other rural census tracts.
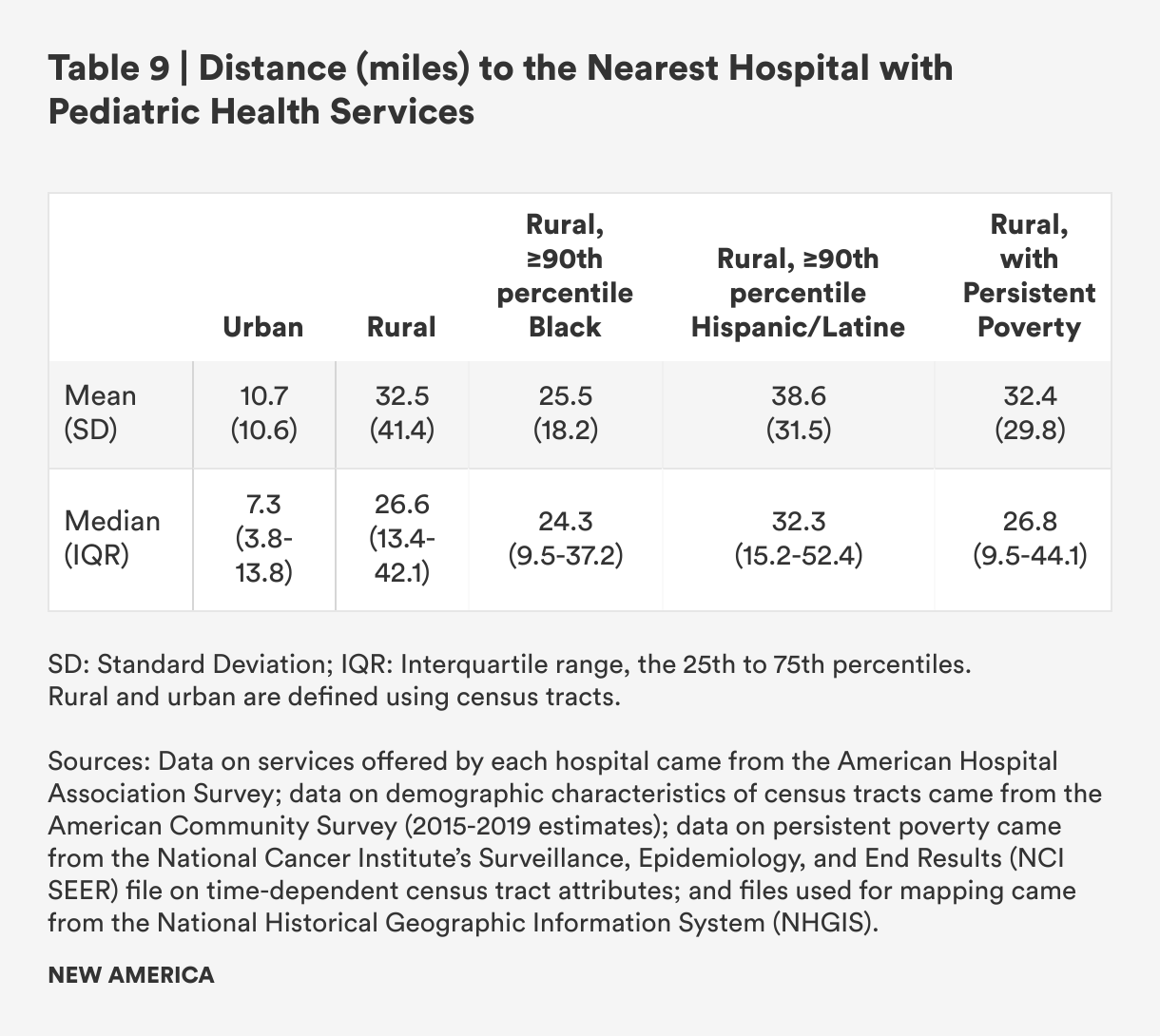
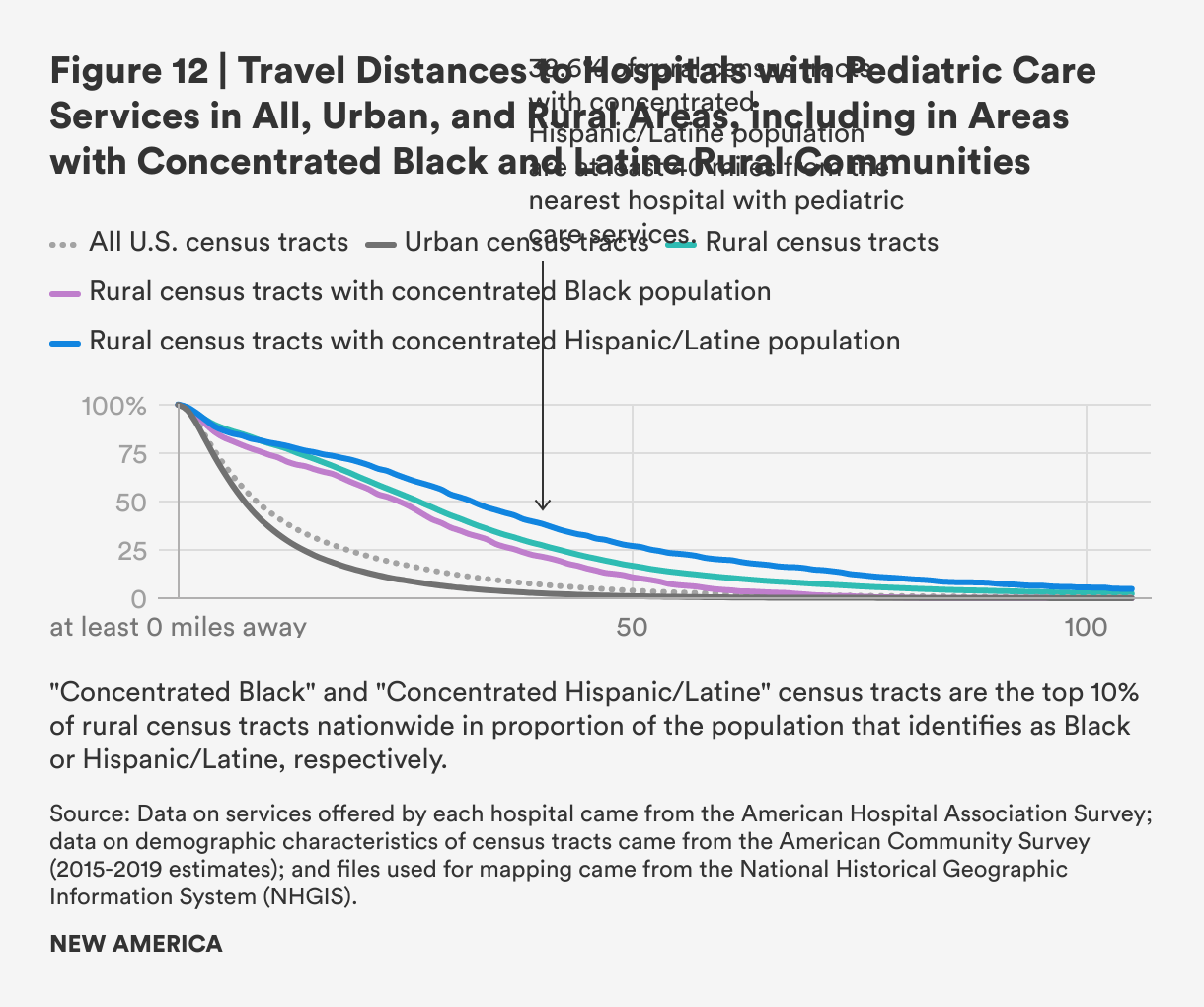
Rural census tracts with concentrated Black populations have substantially lower mean travel distances than rural census tracts overall, but the median is much closer to the median for all rural census tracts. This likely reflects the distribution of census tracts with concentrated Black populations in the South rather than the West. Rural areas with concentrated Hispanic/Latine populations have higher mean and median distances to travel when compared to rural census tracts as a whole, with higher proportions of those areas having to travel in excess of 60 miles for pediatric hospital care, as seen in Figure 12.
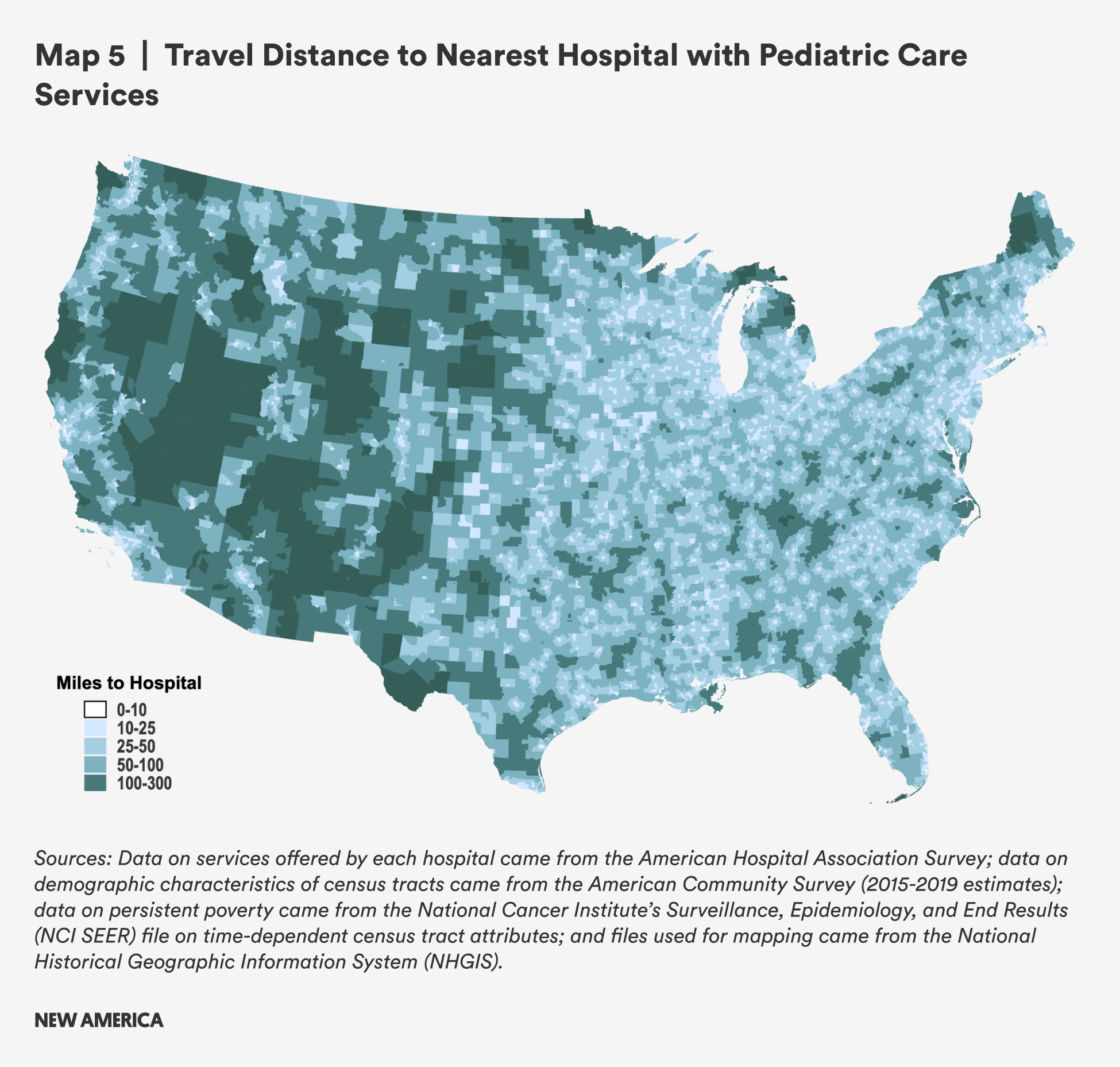
The largest distances are found in the western half of the United States, but areas in northern Maine, Minnesota, and Michigan also have travel distances greater than 100 miles. Many other rural areas still have distances between 50 to 100 miles, which still places a substantial burden on families in need of pediatric health services and especially on working parents.
C. Cardiology Services
Because cardiovascular disease is pervasive in rural communities and is a leading cause of premature death—and because people with cardiovascular disease have lower rates of access to paid sick leave, according to our analysis of NHIS data—we looked at distances to hospitals with cardiac services, including hospitals that report providing adult cardiac care as well as those reporting that they have cardiac intensive care unit. There is variation among these hospitals in the level of cardiac care provided, which means higher level or more specialized services may require further travel than the estimates below.
Table 10 shows that rural census tracts are about four times as far from hospitals that offer cardiology care as urban census tracts: The mean distance from a rural census tract to a hospital that provides cardiology health services is 30.6 miles, compared with 8.0 miles in urban census tracts. The median distances are 22.3 miles and 5.1 miles for rural and urban census tracts, respectively. People in rural census tracts with persistent poverty have similar travel distances.
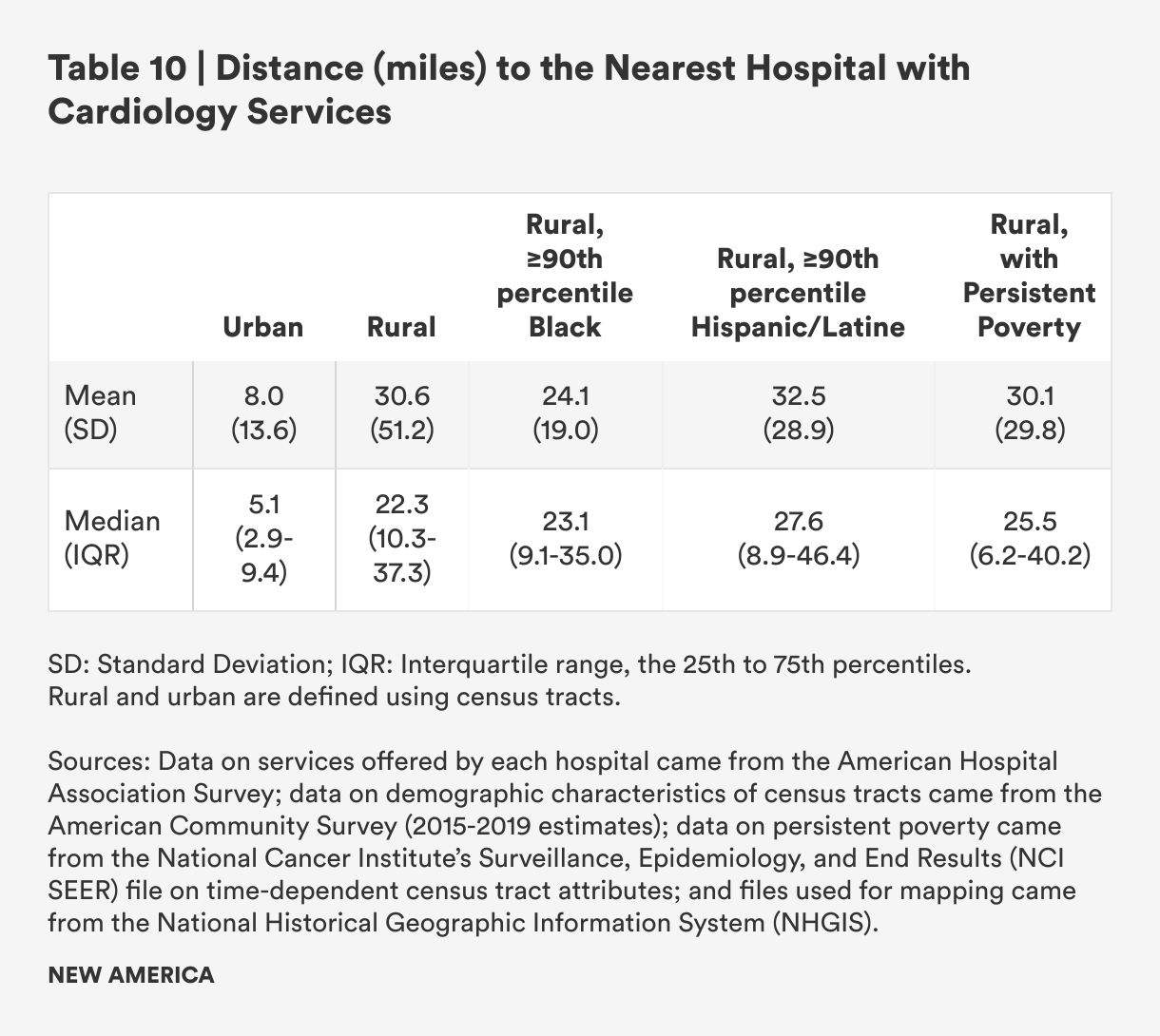
Rural census tracts with concentrated Black populations have lower mean travel distances, but the median distance is closer to overall rural mean distance. Rural areas with concentrated Hispanic/Latine populations have higher mean and median distances to travel when compared to rural census tracts as a whole. As seen in Figure 13, areas with both concentrated Hispanic/Latine and Black populations are more likely to have very short travel distances (<10 miles) but are also more likely to have distances between 25 to 40 miles. A greater proportion of census tracts with concentrated Hispanic/Latine populations have travel distances greater than 50 miles when compared to all rural census tracts—a distance that may be prohibitively far for workers with cardiac conditions who require ongoing or periodic hospital-based care and for caregivers to cardiology patients.

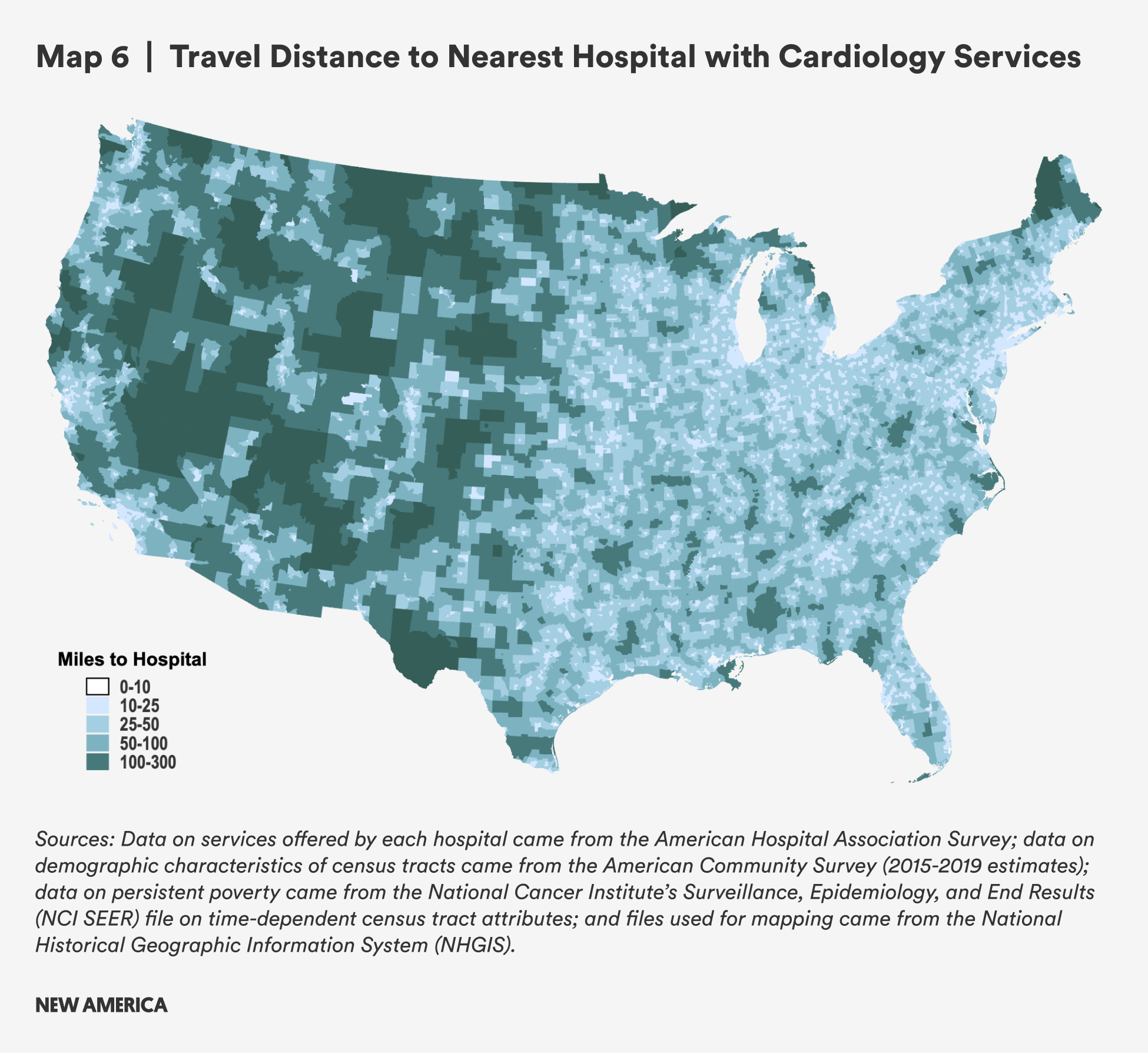
There are many parts of the country which are more than 100 miles from the nearest hospital that provides cardiology services. This map reflects similar findings to previous sections of this report, with people in the West most likely to experience the greatest travel burdens. For cardiac health needs in particular, long distances to hospitals that provide cardiology services may have direct detrimental effects on health outcomes for people who need emergency care. Even among hospitals that provide cardiology services, patients requiring more intensive care may be transferred to other hospitals that may be quite a distance away, so the travel burden on patients and caregivers may be even greater than what is reflected in the map below.6
D. Cancer Screening and Cancer Treatment
Because cancer is a leading cause of rural death, we examined distances to cancer screenings and treatments. Cancer screenings and cancer treatments both require time away from work; workers are more likely to get screenings on time when they have access to paid sick time, and outcomes from disease are better when both patients and caregivers have and use paid time off.7 We examine distances to hospital-based cancer care services in rural communities (defined as providing at least one of optical colonoscopies, endoscopic ultrasounds, and mammograms)—recognizing that longer distances to travel may combine with lack of access to paid leave to adversely affect patient compliance and treatment, or may slow recovery processes due to the fatigue of traveling long distances while working.
1. Cancer Screening
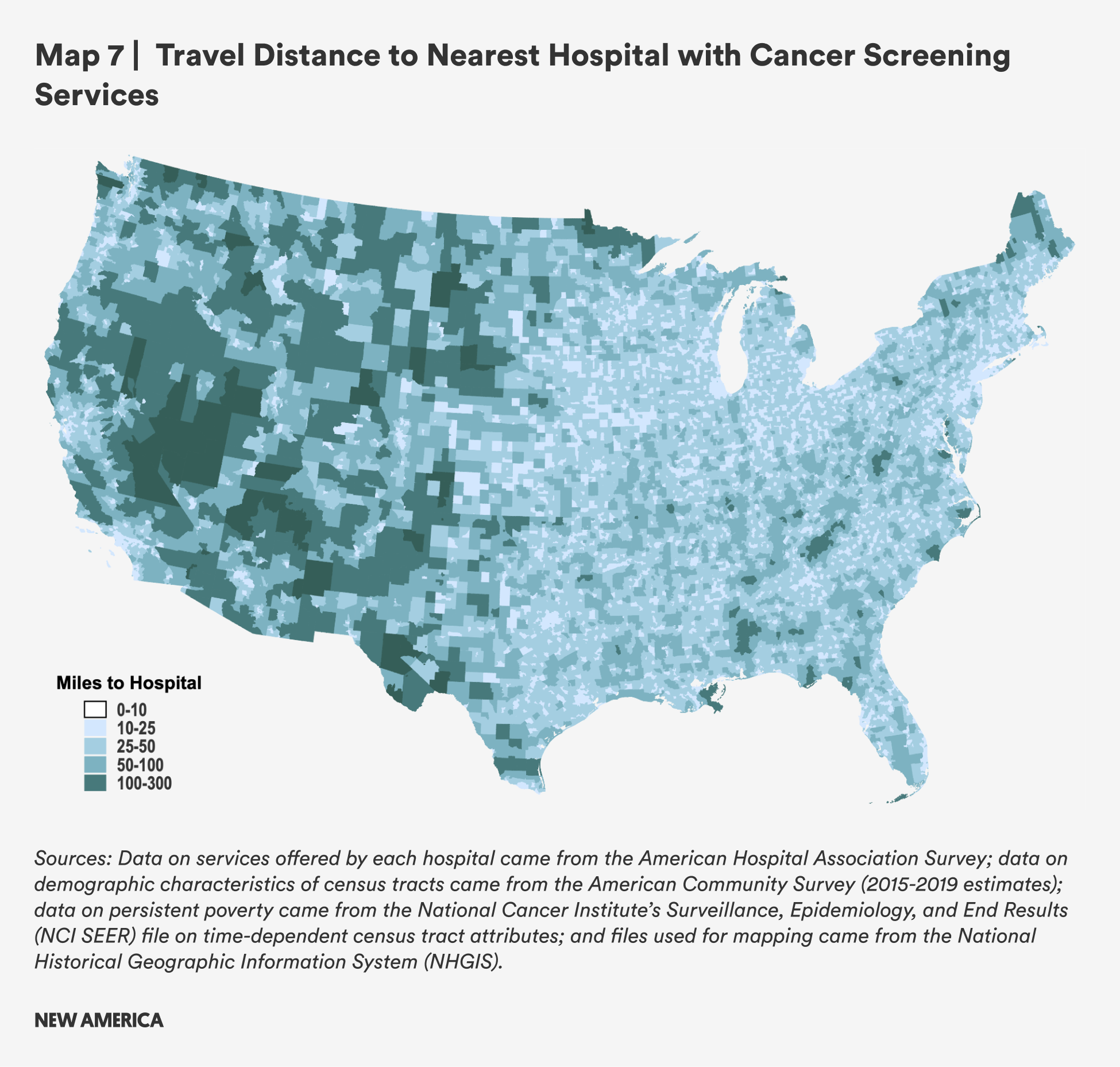
Overall, mean and median distances to hospitals with cancer screening services are further in rural areas than urban ones, but the difference is somewhat smaller than for the other types of hospital-based services analyzed in this report. Rural census tracts are still more than twice as far from cancer screening services as urban ones, and median distances are nearly three times as far (mean: 20.4 miles for rural census tracts vs. 7.4 miles for urban census tracts; median: 14.6 miles vs. 5.0 miles). Rural census tracts with persistent poverty are slightly further away from hospital-based cancer screening services.
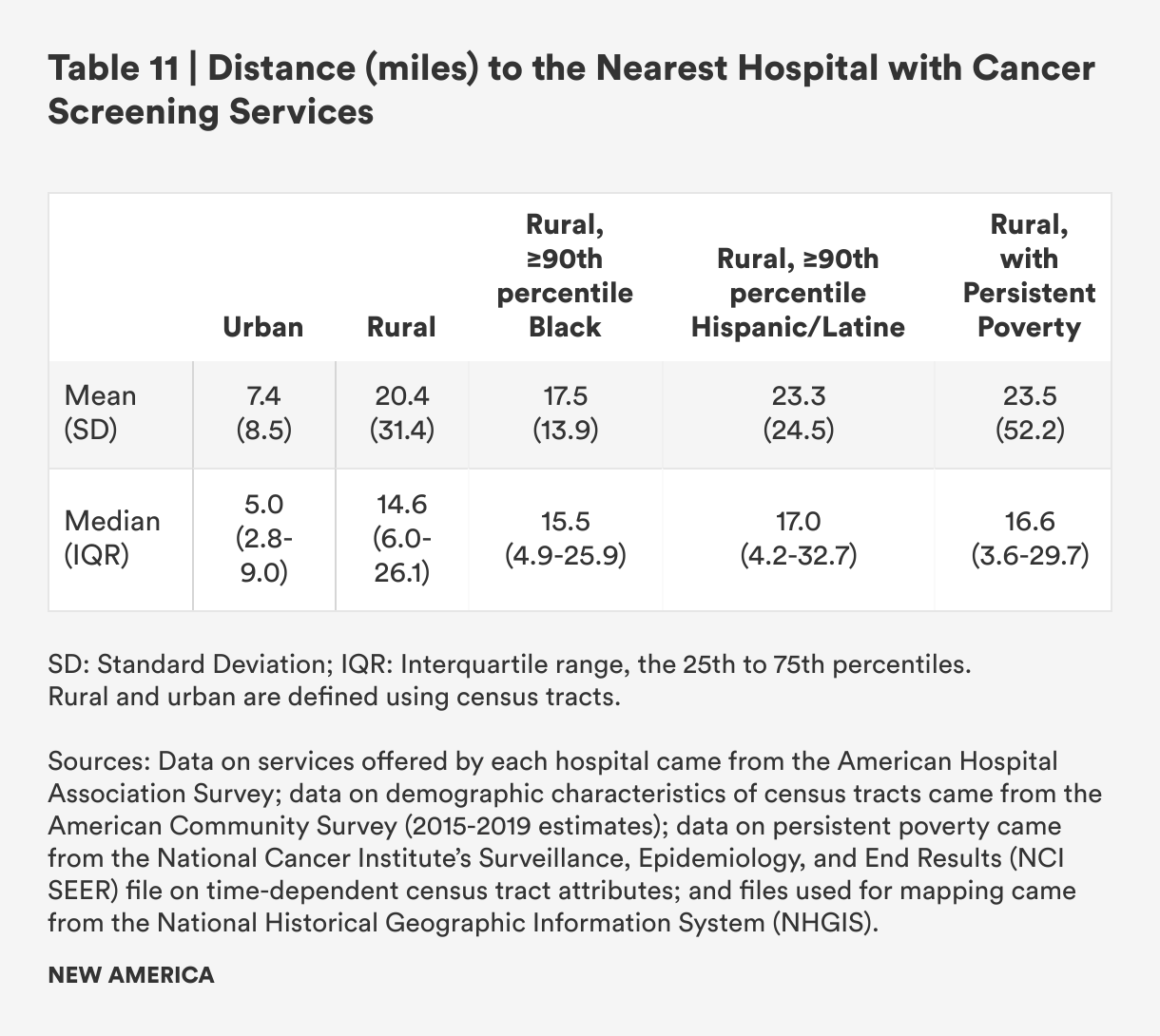
As with other services, distances to hospital-based cancer screenings are slightly larger for areas with concentrated Hispanic/Latine populations and slightly shorter for areas with concentrated Black populations.
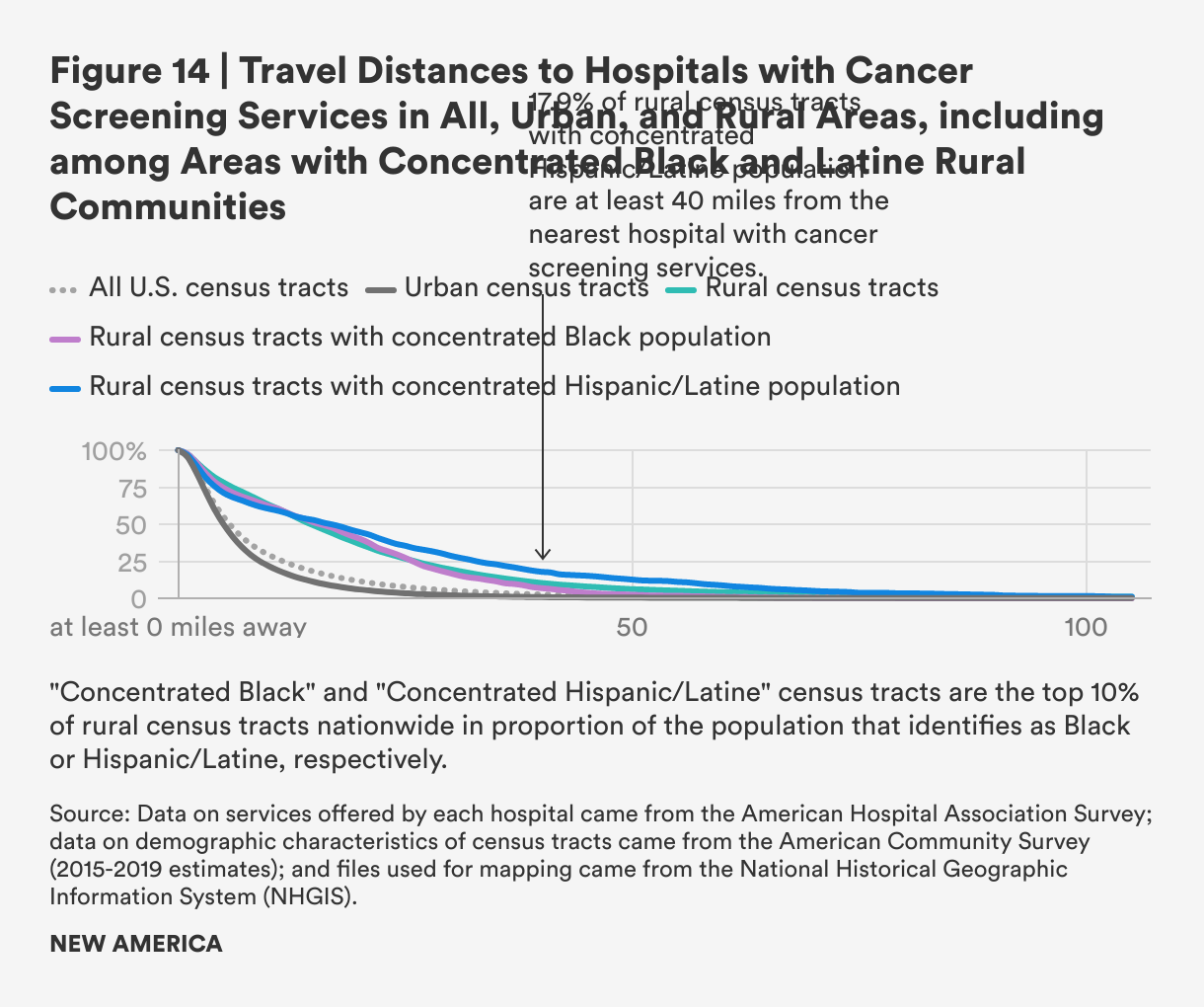
Overall, far fewer rural census tracts have more than 100 miles, or more than 50 miles, between them and the nearest hospital with cancer screening services, compared to other types of health services, yet there are still a nontrivial number places in which residents face significant travel burdens to access these cancer screening services.
2. Cancer Treatment
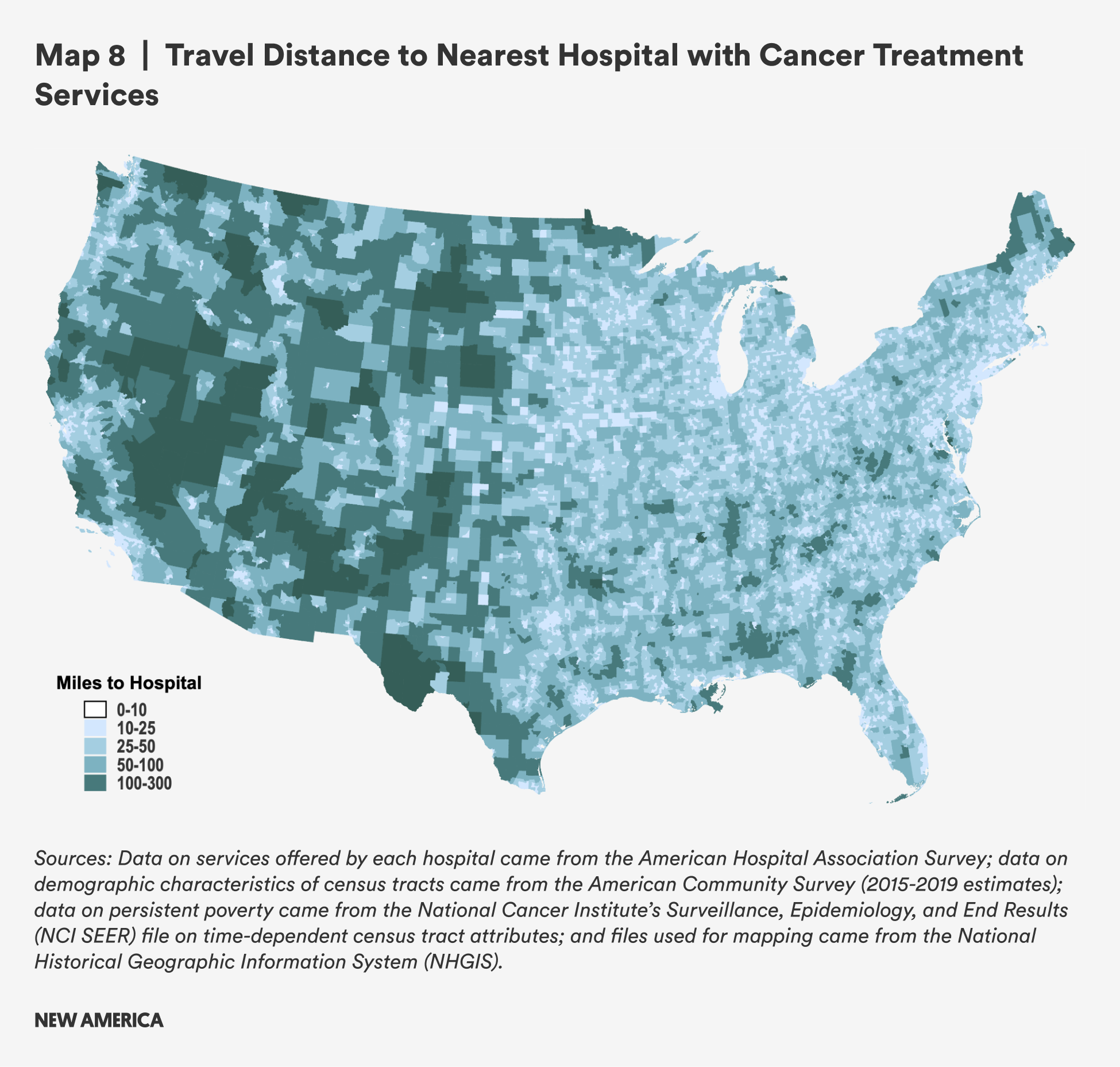
Distances from rural census tracts to hospitals that provide cancer treatment (at least one of chemotherapy, radiation, or other oncology treatment) are greater than distances to cancer screening, with a mean of 26.8 miles to the nearest hospital in rural area and a mean of 20.9, and these are three-to-four times as far from rural areas than from urban ones in terms of mean and median distances, respectively: Urban residents must travel just 7.9 miles, on average, to cancer treatment. Rural areas with persistent poverty have higher travel burdens to those without, with travel distances of about five additional miles to receive cancer treatment at a hospital.

Rural census tracts with concentrated Hispanic/Latine populations have much higher mean (37.3 miles) and median (30.9) travel distances compared to rural census tracts overall. The difference between census tracts with concentrated Hispanic/Latine populations and other rural census tracts is more than 10 miles for both mean and median travel distances, the largest difference for all health care services. This excess distance places greater burden on rural Hispanic and Latine populations who have cancer or are caregivers for people undergoing cancer treatment. The finding for rural census tracts with concentrated Black populations is mixed, with a lower mean distance and a higher median.
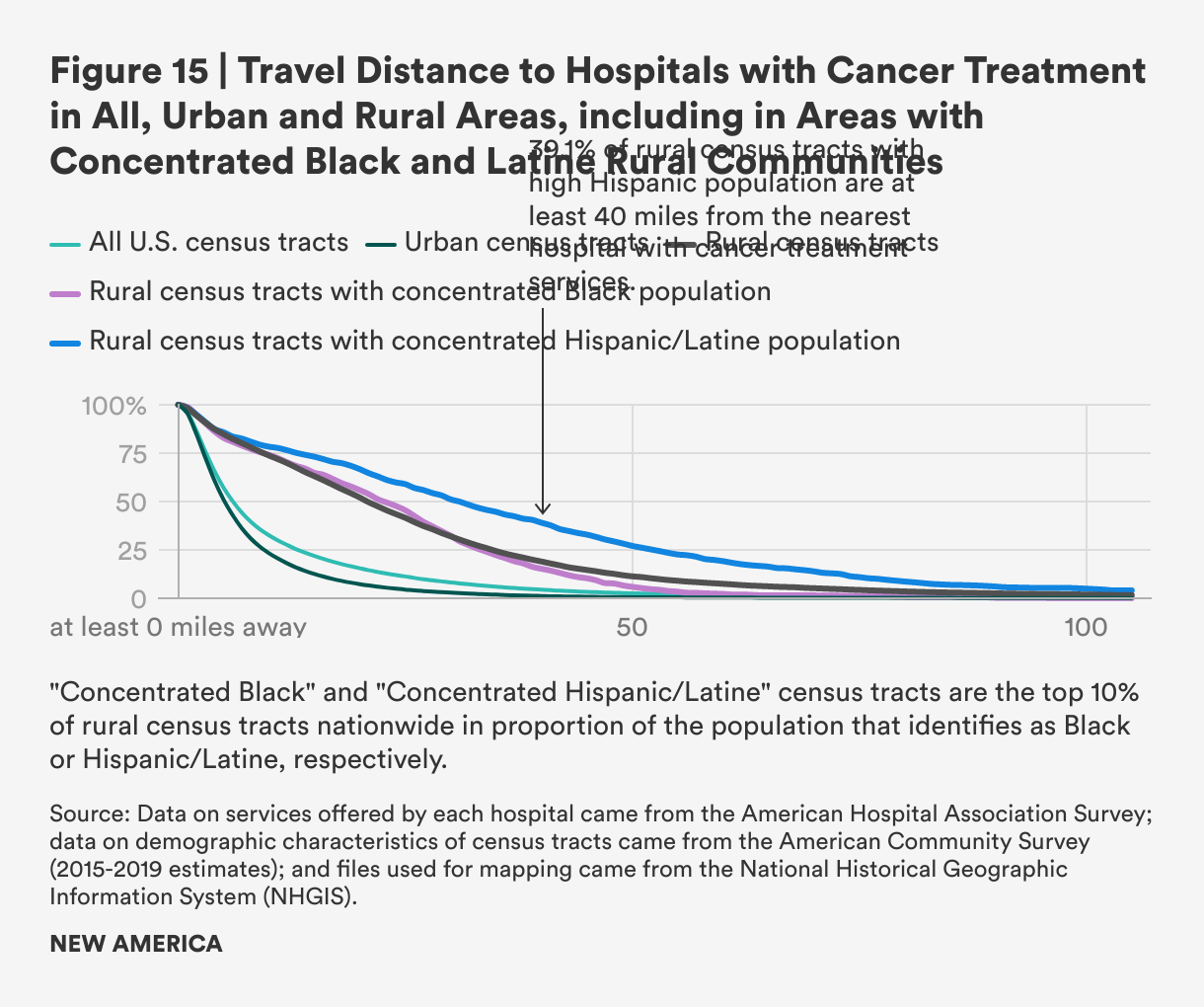
Rural areas in the West and Southwest, and some areas in the northern plains, Midwest and Northeast, face the highest travel burden to hospitals that provide cancer treatment, with much of it more than 100 or 50 miles from care. As many types of cancer care require regular, frequent trips, and care may continue for months, longer distances may be especially burdensome for those undergoing treatment for cancer and the caregivers they may rely on to get to and from treatments.
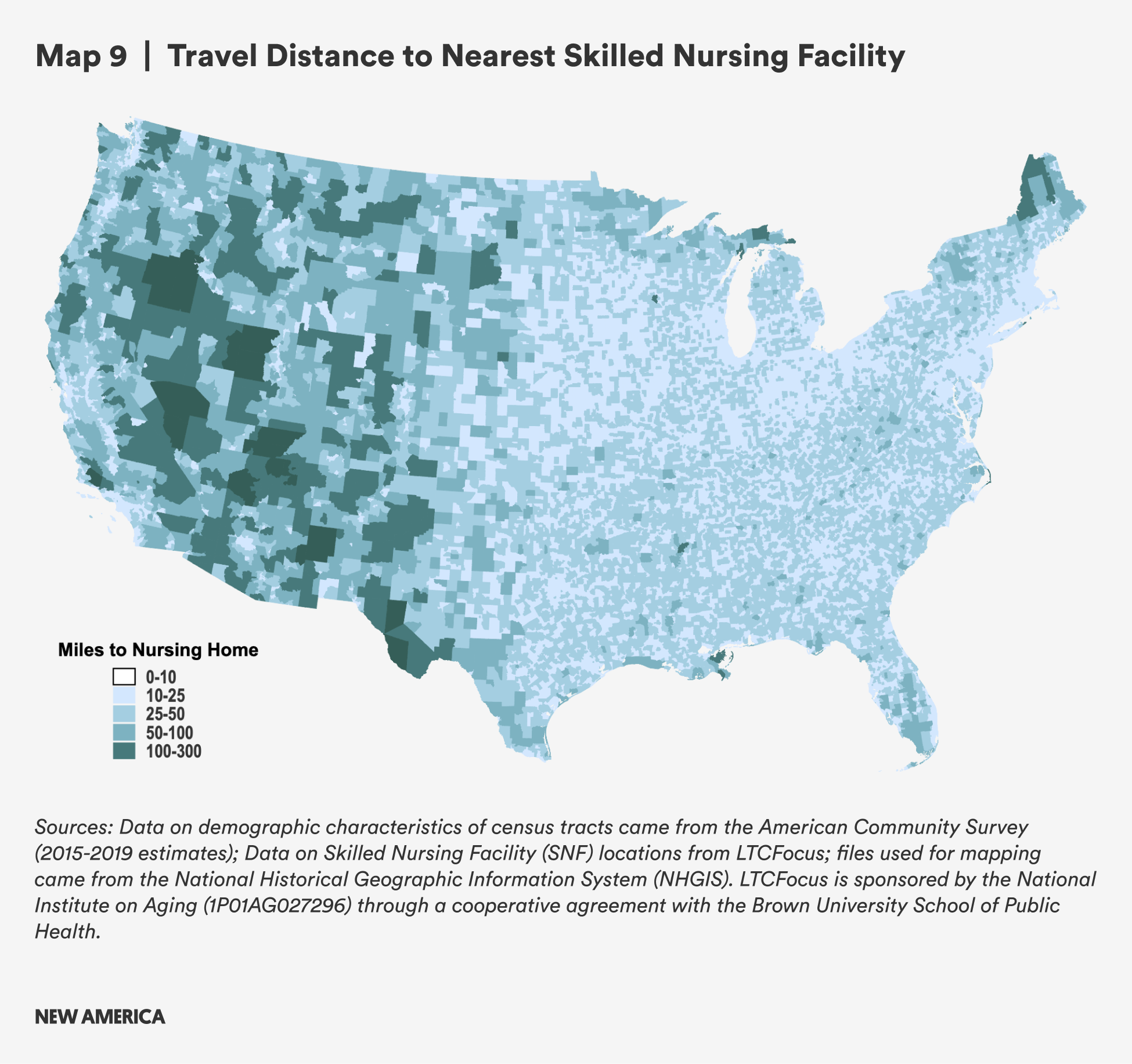
E. Skilled Nursing Facilities
Family caregivers are better able to continue to work when their loved ones are able to access paid care. Skilled nursing facilities (SNFs) are often used after a hospital discharge, but the continued attention of a loved one can be key to better outcomes.
Distances to SNFs are smaller compared to distances to hospitals because there are 14,400 SNFs with location data available, compared with 3,351 hospitals with information on the types of services they provide. To better reflect the vast majority, we exclude 157 census tracts (out of 73,041 tracts where distance could be calculated) in Alaska where the calculated driving distance is more than 500 miles in the results for Table 13, as they significantly skew the mean distance when included. While both mean and median distances are shorter for SNFs than distances to hospitals for any health care services, rural census tracts still have greater mean travel distance by a factor of about three (10.3 miles vs. 3.8 miles) and median travel distance (6.9 miles vs. 2.4 miles), likely creating pressures for family members who are working and providing oversight and care.
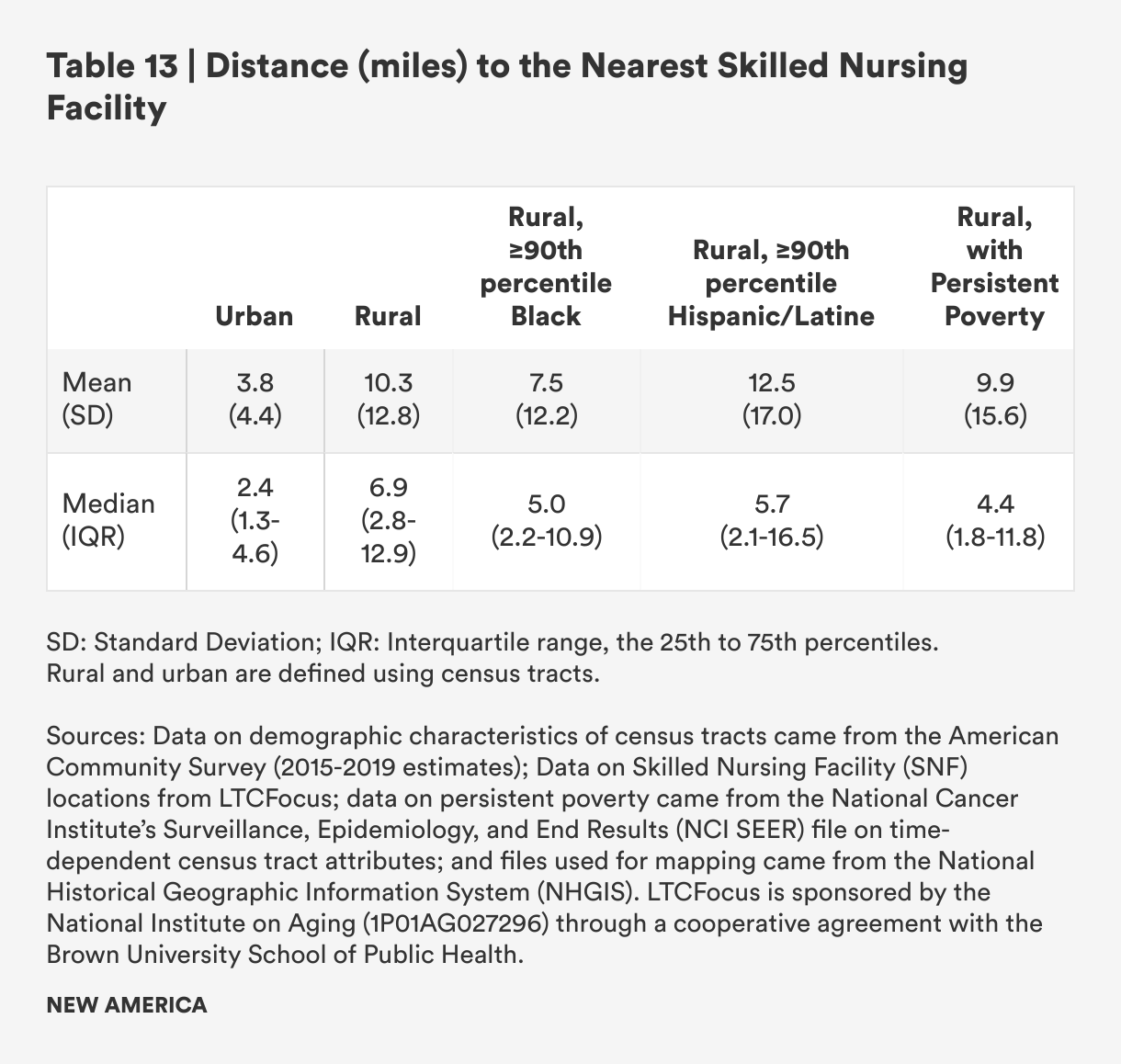
Similar to travel distances to hospitals, rural census tracts with concentrated Black populations have slightly lower mean and median travel distances, while census tracts with concentrated Hispanic/Latine populations have slightly higher mean and median travel distances.

Overall, the travel burden to SNFs is significantly lower when compared to the travel burden for hospital-based health care. There are still areas, however, particularly in the western half of the country, where the nearest SNF is more than 50 or even 100 miles away, making access to skilled nursing services more difficult or entirely inaccessible. These are also likely to be areas where home health services and other non-institutional support services are less accessible because low population density and long travel times between patients may hinder care providers from practicing there. This may increase burdens on family caregivers and make paid employment and caregiving very challenging or impossible.
Citations
- Data limitations mean that we cannot map both access to leave and access to care for the same individuals. Therefore, this report simply adds to the body of literature on each front, to reinforce the point that people in rural communities—especially new parents, people with serious health issues and people caring for loved ones with serious illnesses, injuries or disabilities—would be well-served by new public investments and standards that expand and guarantee access to paid leave.
- We used multiple data sources: data on services offered by each hospital came from the American Hospital Association Survey; data on demographic characteristics of census tracts came from the American Community Survey (2015-2019 estimates); data on Skilled Nursing Facility (SNF) locations from LTCFocus; data on persistent poverty came from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (NCI SEER) file on time-dependent census tract attributes; and files used for mapping came from the National Historical Geographic Information System (NHGIS). LTCFocus is sponsored by the National Institute on Aging (1P01AG027296) through a cooperative agreement with the Brown University School of Public Health.
- Fields et al., “Life off the Highway”; "Tracking the States Where Abortion Is Now Banned,” New York Times, September 23, 2022, accessed October 5, 2022, source
- Stephanie L. Borque, Blair W. Weikel, Mauricio A. Palau, Jennifer C. Greenfield, Anne Hall, Susanne Klawetter, Madalynn Neu, et al. "The Association of Social Factors and Time Spent in the NICU for Mothers of Very Preterm Infants," Hospital Pediatrics 11 (9) (2021): 988-996, source
- Heymann and Earle, Raising the Global Floor.
- Lauren Ziaoyuan Lu and Susan Feng Lu, "Distance, Quality, or Relationship? Interhospital Transfer of Heart Attack Patients," Productions and Operations Management 27 (12) (2017): 2251–2269, source; Daniel Bechtold, G.G. Salvatierra, Emily Bulley, Alex Cypro, and Kenn B. Daratha, "Geographic Variation in Treatment and Outcomes Among Patients With AMI: Investigating Urban-Rural Differences Among Hospitalized Patients," Journal of Rural Health 33 (2) (2015): 158–166, source; Theodore J. Iwashyna, Jeremy M. Kahn, Rodney A. Hayward, and Brahmajee K. Nallamothu, "Interhospital Transfers Among Medicare Beneficiaries Admitted for Acute Myocardial Infarction at Nonrevascularization Hospitals," Circulation: Cardiovascular Quality and Outcomes 3 (5) (2010): 468–475, source.
- Lucy A. Peipins, Ashwini Soman, Zahava Berkowitz, and Mary C. White, "The lack of paid sick leave as a barrier to cancer screening and medical care-seeking: results from the National Health Interview Survey," BMC Public Health 12 (2010), source; Public Opinion Strategies, Interested Parties Memorandum.