
Table of Contents
Early Education and Care as a Path Towards Equity
Young children of immigrants lost access to many critical interventions beyond daily lesson plans. For the children of immigrants, the impacts of COVID-19 on childcare and education are compounded by structural inequalities that long preceded the pandemic. Distance learning prevents teachers from engaging with undocumented students’ trauma and anxieties. Immigrant students additionally cannot access hot meals and caring adults, including teachers, school counselors, and nurses, who might be able to mitigate their losses and challenges.
Extensive studies in economics, neuroscience, medicine and developmental psychology all conclude that early childhood investments can benefit children, parents, and nations because early childhood, beginning in infancy, allows profound opportunities to advance children’s skills in reasoning, language acquisition, and problem solving. Public investments in early childhood education bring substantial returns in children’s educational trajectories and a more skilled future workforce because early education improves children’s educational performance and attainment, improves health, decreases crime, and improves long-term economic self-sufficiency and returns.
The importance of early education is widely recognized internationally. According to the United Nations Educational, Scientific and Cultural Organization, early childhood care and education “is one of the best investments a country can make to promote human resource development, gender equality and social cohesion, and to reduce the costs for later remedial programmes. For disadvantaged children, [early childhood care and education] plays an important role in compensating for the disadvantages in the family and combating educational inequalities.”
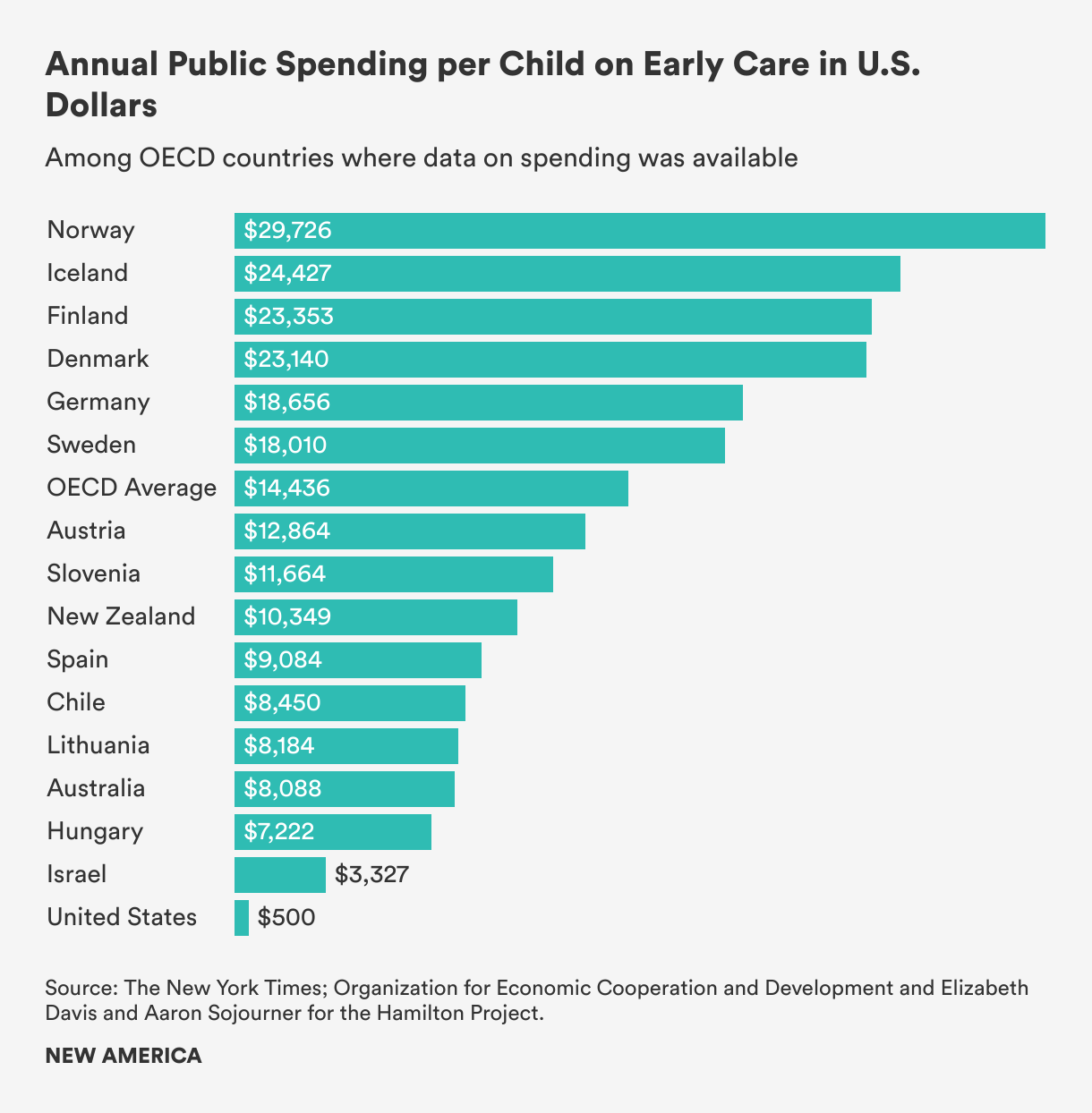
Despite the research on the dramatic development of children in the first few months and years of life, the United States lags significantly in investment in young children’s education and care compared to other wealthy nations. The New York Times shows that the United States spends less than 0.2 percent of its GDP (gross domestic product) on childcare for children two and under—which amounts to about $200 a year for most families, in the form of a once-a-year tax credit for parents who pay for care—while other wealthy countries in the Organization for Economic Cooperation and Development spend an average of 0.7 percent of GDP on toddlers, mainly through heavily subsidized childcare.
Access to early education is unequal. Differences in access to and utilization of early care and education programs depend significantly on income and educational attainment of the parents. Participation in early childhood education is high among children from highly-educated and high-income families. Since the 1970s, children of less-educated mothers are still less likely to attend preschool. In the United States, 90 percent of families in the top 20 percent of income distribution are already purchasing preschool education for their children. In contrast, among families in the lowest 40 percent of income distribution, fewer than 60 percent of children are enrolled in preschool education. Families below the federal poverty level paid an average of 30 percent of their income in childcare costs compared to 8 percent among non-poor families. This inequity produces gaps in cognitive, linguistic, social, and emotional skills that become evident well before children enter kindergarten.
For years, early childhood education has been recognized as a meaningful avenue to compensate for the disadvantages in the family and reduce educational inequalities. In addition to promoting the development of children, quality and sustained care can help immigrants’ children adapt to a new socio-cultural environment, mitigate the impact of trauma, and offer critical wraparound services. Learning environments attentive to safety and trust through consistent routines and expectations can restore a child’s feelings of control after adverse experience.
Early Head Start, a federal program launched in 1996, provides services for at-risk pregnant women, new mothers, children ages zero to three, and their families, and focuses on positive parenting and home environments and children’s developmental outcomes, has shown positive results for cognitive development and language acquisition. Children who participated in Early Head Start showed less aggressive behavior, greater vocabulary and language development, and higher cognitive skills upon the program’s completion, and parents who received Early Head Start services showed greater engagement during play and greater support for language and learning development at home. Head Start, which serves low-income three- and four-year-olds, improves educational outcomes (increasing the probability that participants graduate high school, attend college, and receive a post-secondary degree or certificate) and promotes social, emotional, and behavioral development (adulthood measures of self-control, self-esteem, and positive parenting practices).
Attendance in early education programs in general, and Head Start in particular, has been shown to raise reading and math test scores for children of immigrants. Head Start participation also increases positive parenting practices for each ethnic group and for participants whose mothers did not have a high school diploma or equivalent when compared with the outcomes of children who went to a preschool other than Head Start. In addition to offering early childhood development services, Head Start programs provide comprehensive assessment and services for the whole family, including education, nutrition, and health/mental health care, and even employment of some refugee parents by Head Start agencies.
Barriers to Early Learning and Care for Children of Immigrants
Like Justine’s and Zahra’s families, the majority of children of immigrants do not use center-based childcare, despite the well-documented benefits of early learning services on children’s school readiness and long-term cognitive, socioemotional, and educational outcomes. The majority (53 percent) of children of immigrants under six receive childcare from parents. Only 17 percent of children of immigrants are in center-based care. The use of center-based care is lowest among immigrant parents with less than an eighth-grade education, as compared with approximately 60 percent of the general population. These children are also less likely to attend preschool and Head Start programs.
There are a number of reasons why immigrant families enroll less in early childhood education overall. Some of these reasons are the same as those faced by all parents: costs, waiting lists, locations, service hours that do not cover the full workday, and lack of information about available programs. As mentioned above, immigrant parents are more likely to have low incomes and nonstandard work hours than U.S.-born parents, and thus, especially affected by schedules. Because transportation is a major issue as many rely on public transportation, location becomes another difficult calculus of scheduling. Poor immigrants tend to live in segregated neighborhoods with fewer childcare services. Children who live in areas with the highest share of foreign-born parents are about 13 percent more likely to live in a childcare desert than those who live in areas with the lowest share of foreign-born parents. In addition, immigrant workers are 15.7 percent more likely to work during nontraditional hours and 25.2 percent more likely to work weekends compared to similarly situated U.S.-born workers. Only 8 percent of childcare centers are open during these times, making family, friend, and neighbor (FFN) care—also referred to as kith and kin care, relative care, informal care, home-based care, and license-exempt care—all the more essential for immigrant families.
Obstacles such as parents’ language barriers, logistical barriers to enrollment, and lack of comfort with available programs can all prevent immigrant families from enrolling their children in early education programs. A study on 2,500 immigrant families found that families relying on parent care were less proficient English speakers, less educated, earned less money, and had mothers who worked less. Maternal employment predicted home-based care usage much more strongly than the availability of care centers, suggesting either a preference for home-based care over center care that is unique to immigrant families or that the likelihood of performing low-skill work makes center-based care less accessible due to its cost and inflexibility of schedule. This study also shows that the decreased availability of non-English speaking childcare providers increased the probability of parent care. The decrease in the availability of non-English speaking providers within 20 miles of families’ homes lowered the probability that children would experience home care, center care, or Head Start versus parent care by 35 percent, emphasizing the significance of language continuity in the choice of early education and care.
Like Zahra Hasmi, many refugee families are isolated from the general population, and therefore, do not know about early education options. Furthermore, the violence in their home country produces anxiety around separation from their young ones. Zahra Mohammed, 22, who has been in the United States for about a year, states that her three-year-old daughter is too young to leave her care. She adds that she might let her daughter attend preschool after she learns "American rules." Mohammed’s unease about preschool became further explained when her mother expressed worries about the possibility of Mohammed being kidnapped when the interview ran a little over an hour. Bibi Abdullah, 26, who has been in the United States for five years, describes the belief that she is safe as the most difficult adjustment in the United States. On one occasion, she ran a red light and sped off because she was so certain that the car behind was following her. She didn’t notice the police siren chasing her until one officer came at her from the front. She recalls sleeping a few hours at night, holding tightly onto her daughter and showing up at her daughter’s school to check on her safety. Bibi said it took her over a year and interactions with many supportive people to let her guard down.
Furthermore, many immigrant parents express fear around center-based care. They worry that child rearing practices, which may be historically rooted and culturally normative, may place them in vulnerable positions in the United States where they may not be viewed as acceptable. They also worry about being tracked, monitored, or reported. Additionally, deep-seated fears for some around legal status increase hesitance to engage in services. The immigration status of family members influence use of Head Start and Child Care and Development Block Grant, even though Head Start has no citizenship restrictions and the Child Care and Development Block Grant funding is exempt from verifying the immigration status eligibility of any child. The Child Care Development Fund is a federal and state partnership that provides childcare assistance, in the form of subsidies, to low-income, working families with children under age 13. These subsidies help low-income families to access early education and care for their children and support parental work or participation in education and training activities. While the grant regulations make it clear that childcare subsidies target children, and therefore that their parents’ immigration status cannot be considered in qualifying, of the 13 states that contain 80 percent of the Latinx population, 12 requested the Social Security numbers for household members in Child Care and Development Block Grant applications, and seven of these states did not indicate that providing the Social Security numbers was optional. The lack of clarity can deter immigrant families from applying even though their children qualify.
Local context around immigration and parents’ prior experiences with other government programs can affect the relationship between parents and early childhood education providers. For example, immigrants may have interactions with public officials that lead to mistrust of government institutions, including school-based pre-kindergarten programs, particularly in cities where new immigration enforcement laws are passed.
Making Early Education and Care Accessible
Because center-based care and Head Start have shown to benefit preschool-age children and prepare them for school, both psychologically and scholastically, the underutilization of publicly funded early education programs by immigrant families is troubling. Access to high-quality early childhood education and care is critical for minority and low-income children, who are often at greatest risk of falling behind. Compared with children with U.S.-born parents, children of immigrants begin school, on average, with fewer of the early literary, numerical, and language skills that support future academic success. The children who need sustained and quality childcare the most in order to break systematic barriers, such as low-income, limited English proficiency, and low-education, do not have access to it.
As mentioned above, the potential of universal pre-kindergarten and expansion of quality and affordable childcare benefit will not reach children of immigrants if policies fail to address the many reasons that prevent immigrants from using childcare programs: English language and literary barriers, the fear of being a “public charge,” concerns of racism and cultural bias, transportation, cultural responsiveness, and non-traditional hours. Publicly funded centers that continue to reflect a white dominant standard of quality without addressing lack of racial diversity, institutional racism, language barriers, and shortage of cultural brokers will alienate immigrant families.
In addition to mitigating structural barriers, including language access, scheduling, location, transportation, and cost—factors that shrink initial enrollment and continued attendance among many immigrant families—programs can simplify enrollment, initiate cultural aware outreach, advance staff recruitment and ongoing training, and develop trusting relationships with parents in order to reach more immigrant families. All of these suggestions have been successfully carried out and can be adapted nationally with adequate funding and initiatives.
Data Collection
The first step in connecting immigrant families to early learning programs is to learn who the immigrant families are in a community, where they are, the extent to which they enroll in early education programs, and the issues they face that affect their willingness to access these programs. All Head Start grantees are required to conduct community needs assessment every three years to determine the demographic makeup of eligible families and kids, including their numbers, geographic locations, and racial and ethnic compositions. These assessments also study local concerns and community resources to identify and prioritize families most in need. Like Head Start, Washington state requires local pre-kindergarten programs to conduct community needs assessments every three years. Providers are asked to calculate the number of children by race and ethnicity, migrant or seasonal farmworker status, and home language, among other factors. Some school districts in New Jersey are likewise required to conduct community needs assessments. In other states, regional governing bodies determine the characteristics and needs of children in their service area. For example, North Carolina depends on local pre-kindergarten advisory committees that identify children in the community who would qualify for pre-kindergarten and work with the community to identify ties to those groups. Data must be disaggregated to prevent upholding stereotypes and overlooking some groups. For example, over 17.5 million members of nearly 50 different races and ethnicities are categorized as monolithic Asian American and Pacific Islanders and hailed as the “model minority.” As a result, communities such as Hmong Americans, who are less likely than the average resident to have a household income over $50,000, be employed, or be a college graduate, are at substantial risk of being underserved by local, state, and federal governments. Additionally, Hmong Americans, unlike some other Asian Americans, endured war, refugee camps, and harrowing migration, and thus, experience many traumas.
Simplify Enrollment
Programs serving diverse populations have worked in various ways to streamline and facilitate the enrollment process for families. This can involve simplified application forms, enrollment assistance, and flexible times and locations for enrollment. Some programs design processes to facilitate immigrant inclusion, such as not asking for parents’ or children’s Social Security numbers; translating forms, related web sites, and informational materials into common languages spoken by immigrant parents; allowing flexibility in the types of proof of residence and other documentations; and not requiring proof of income unless necessary.
Programs can offer to help families with health screenings and immunizations requirements by connecting families to partners who provide low-cost or free healthcare to young children. This helps immigrant families who struggle to afford the cost of taking children to the doctor since immigrant families are more likely to lack health insurance than U.S. families overall. Programs can offer a centralized registration to include interpreters, health providers who can complete required health screenings, and representatives from social service agencies who can respond to any broader family issues that might arise in the enrollment process.
Outreach, Staff Recruitment, and Training Activities
A recent analysis of infant and toddler early learning guidelines in 21 states found a lack of attention to the developmental and learning needs of dual language learners. States can pay for ongoing training that is intended to help providers and teachers work towards improved cultural competency. States can also work with childcare resource and referral agencies to create professional development plans that incorporate culturally and linguistically appropriate training and partner with community-based organizations with expertise in providing training services to English learning childcare providers. Additionally, states can offer scholarships and grants for diverse providers to attain education and training or increase compensation for bilingual childcare providers to retain a diverse early childhood workforce.
Teachers and staff at all levels of diverse racial, ethnic, and linguistic backgrounds need to be recruited and supported to work with diverse babies and toddlers. States can require programs to report on their plans for outreach in the underserved communities, on how they get the word out about the program to at-risk populations, on development and implementation of a coordinated process for recruiting, identifying, and enrolling at-risk young children, and on written plan for working with children and bilingual families. In light of the rapidly changing immigration policy contexts at local and national levels, offering cultural sensitivity training can promote trust from families from all national origins.
Parents can be reached directly through information packets for new parents in multiple languages that discuss quality childcare, availability of childcare assistance, and other benefits and services for their children. Several states offer kits to parents of all newborns in the state before they leave the hospital or birthing center, with information and resources to help parents care for their child, including tips about child development, health and safety, quality childcare, and school readiness only in English, positioning immigrants as a marginalized community. First 5 California, as an alternative example, offers kits available in English, Spanish, Chinese, Korean, and Vietnamese. These kits can also be distributed through clinics, doctor’s offices, community centers, and libraries.
Word of mouth from family, friends, and community organizations remain the primary source of information about early education and care services. States can provide funds to community-based organizations and immigrant-serving nonprofits to develop general information about childcare programs in appropriate formats and in the primary languages of immigrants in their communities. In some cases, policymakers have sought to place early education programs in targeted community-based organizations to reach immigrant groups that are under-enrolled in prekindergarten. Georgia, for example, is currently working to place pre-kindergarten programs within community-based organizations. The Wisconsin Department of Workforce Development, as another example, contracts directly with a migrant services provider, United Migrant Opportunity for bilingual childcare services that meet the needs of migrant and seasonal farmworkers.
In order to introduce early education and care to immigrant families, who are unfamiliar with non-parental care for young children, care systems need to work closely with refugee resettlement centers and community and religious leaders. Meet immigrant families where they already go, such as festivals and gatherings and at apartment complexes with large immigrant populations. Programs can pass out information or post flyers at popular locations, such as groceries stores, laundromats, doctor’s offices, faith-based organizations, refugee resettlement offices, libraries, English as a Second Language classes, adult education, and citizenship classes. Programs should work with staff at those agencies to explain available prekindergarten programs and how parents can find out more information and apply. Because WIC is available to children up to age five, regardless of parents’ immigration status, it is a particularly good location for reaching pre-kindergarten-eligible children of immigrants. Newark Public Schools has used more intensive in-person outreach through door-knocking campaigns, organizing community leaders to lead teams in door-to-door outreach to promote prekindergarten programs.
States that have done a great job at enrolling children of immigrant families have explicit state requirements to do so:
- Florida has a constitutional amendment requiring pre-kindergarten access for all four-year-olds and now has an 80 percent enrollment rate.
- Maryland has a state law that low-income children who qualify for free or reduced price lunch must be guaranteed a seat in a pre-kindergarten program from the day they show up to enroll, without a waiting list.
- New Jersey has 30 low-income school districts that are required to establish public, free pre-kindergarten programs, and must reach a target of enrolling 90 percent of four-year-olds in the district in pre-kindergarten. Because children of immigrants make up an overwhelming share of the overall population of children in these districts, programs in these communities apply substantial effort into mass media and in-person outreach in English and Spanish to reach all families in the area.
Trauma-informed Care
The ability for early education programs to reach large numbers of young children makes it uniquely apt as a critical context in which trauma-informed care can be delivered. However, the lack of training, resources, and racial bias has led to three- and four-year-old children being expelled at significant rates—over three times—than those in kindergarten through 12th grade. As a result, mental health issues that lead to challenging behaviors remain unaddressed. Young children are removed from all the benefits associated with early education, placing even more burden on parents to deal with a problem that is largely systematic as a personal failing. Moreover, Black children attending state-funded pre-kindergarten are twice as likely to be expelled than white children. Because one-in-10 Black people in the United States are immigrants, it is imperative to note that there is no such thing as a “Black issue” versus “immigrant issue.” Racial bias can be amplified with young children of immigrants whose culture and native language may be foreign to early education teachers and staff. Moreover, few practitioners have the skills needed to recognize and implement trauma-informed interventions within early childhood settings.
The high expulsion rate also indicates that parents and caregivers need help, starting from birth, to support the social and emotional development foundational for learning, future relationships, and school readiness. Work conditions, including low salaries, long hours, and high teacher-to-child ratios, may contribute to teachers feeling stressed or depressed, affecting their behavior management skills or tolerance for potential symptoms of trauma. As a result, supporting staff wellness is critical to any trauma-informed approach in early education programs. Staff needs access to early childhood mental health consultation to assist teachers, enforcement of lower student-teacher ratios, reasonable hours, and support to address secondary stress and related turnover.
Nationwide, early childhood programs are being encouraged to implement policies to reduce and eliminate preschool expulsion. The recently revised Head Start Program Performance Standards clearly prohibit expulsion due to children's behavior. Additionally, policymakers and providers are more knowledgeable about trauma-informed practice, which recognizes that children's history of trauma impacts their development, learning, emotions, and behavior.
Government funding and initiatives are needed to promote coordination of services that provide comprehensive training for staff, create safe and supportive early learning environments, and address cultural and linguistic needs. Adopting a trauma-informed philosophy requires a paradigm shift that begins with understanding that challenging behaviors are normal reactions to trauma and not intentional misbehavior. Programs such as Early Head Start and Head Start with access to infant/early childhood mental health consultation report less expulsion. In addition to general trauma-informed training, early education programs need to invest in language access, cultural-sensitive training, and understanding of challenges particular to young children of immigrants. Wraparound services are necessary to strengthen families, promote relationships, decrease parental stress, and improve family safety and financial security.
Nationwide, early childhood programs are being encouraged to implement policies to reduce and eliminate preschool expulsion. The recently revised Head Start Program Performance Standards clearly prohibit expulsion due to children's behavior. Additionally, policymakers and providers are more knowledgeable about trauma-informed practice, which recognizes that children's history of trauma impacts their development, learning, emotions, and behavior.
Build Positive Relationships with Parents
Another, less named, resistance towards early education is the concern that young children would forget their families’ cultures and languages. Malaly Hermat, 44, an Afghan refugee who now has U.S. citizenship, does not want her four-year-old daughter Sansa to attend preschool regardless of its potential benefits. Hermat married when she was 13-years-old and raised six children without preschool in Afghanistan. She has been following her own customs of raising her children and takes pride in her way of life. Hermat’s story reminds community organizers and policymakers that refugees do not flee without looking back to their home. Sansa is an outgoing and bossy child, whose confidence is no doubt a result of the doting attention of her mother.
Families (including chosen families) are young children’s first and most important teachers. Developmentally appropriate practices for young children should be informed by knowledge of young children’s social and cultural contexts, according to the National Association for the Education of Young Children. Strong partnerships between parents and providers enhance children’s social, emotional, and cognitive development. In Sansa’s circumstance, valuing the home culture and language might be the only way to draw her to preschool.
Engaging parents through reciprocity, trust, honesty, respect, and sensitivity is also the basis of a trauma-informed culturally responsive relationship with families. Honor diverse family structures and recognize and strive to counter the historical bias toward idealizing (and conversely blaming) biological mothers as primary caregivers. Early education programs can help families nurture their child’s social and emotional development by connecting them with pediatricians, parenting groups, and home visiting services.
Because parents and caregivers may also be trauma survivors and express their own fight, flight, and freeze survival responses in their interactions with teachers, teachers must respond to resistance or lack of engagement from parents with empathy, patience, and a lack of judgment. Teachers need to be prepared that it may take additional time to build trust with parents as their own histories may lead them to struggle to build trust in relationships with other adults. Families are best supported in facilitating their children’s development and mental health when services are available in their native languages.
Orientations, home visits, and open houses can build ties between schools and immigrant parents to the extent that parents feel comfortable participating and have positive interactions during these occasions. Schools offer parents leadership and advisory roles. Parent-led outreach is particularly effective, since they can communicate to one another in their home language and in a culturally appropriate manner. The Community Action Project in Tulsa, Oklahoma, for example, has a “captain” program that provides gift packs to parents who successfully recruit other families for the Head Start program. Portland Public Schools in Maine hires immigrant parents to serve as outreach workers. In Chicago, several agencies and organizations have collaborated to create a Head Start Ambassador program, in which parents are trained to reach out to Head Start-eligible families and encourage them to enroll.
Establishing relationships with parents can also create a sustainable early education workforce, in which eight in 10 providers cite a staffing problem, and half of providers stated hiring as harder than before the pandemic. Childcare centers also struggle with retention with a roughly 30 percent turnover rate each year. And yet, Parents In Community Action, Inc. (PICA), the federally designated grantee that operates Head Start programs, has staff members who have been there for decades. Over 70 percent of its staff are parents whose children are in the program or have graduated from the program. Following a two-generation approach, PICA offers a number of training programs to help parents learn new skills, gain hands-on work experience, and prepare for the future.
Family, Friend, and Neighbor Care
Family, friend, and neighbor (FFN) care is the oldest and most common form of childcare among all families. Families may choose FFN care because it is the option that is most comfortable and familiar, most flexible, most affordable, or provides children with the most individualized attention. In 2016, 60 percent (12.8 million) of the 21.4 million children under age six were in some type of regular childcare arrangement in a typical week. Since early 2020, due to the COVID-19 pandemic, FFN care became the only option for many families. Families, hesitant to enroll their children in large group settings, increasingly sought out FFN care during the pandemic. By early September, the percentage of households using FFN and other home-based care exceeded pre-pandemic levels. Although FFN providers outnumber center-based providers and serve more children, FFN care is largely undervalued by federal and state policymakers.
Justine’s preference for her children to be cared for by her aunt reflects the prevalent use of FFN care among immigrant populations. In addition to lower cost and flexibility in location and service-hours, these caregivers often share language and culture with families of the children in their care, and thus, offer a trusted, safe, and high-quality experience that is responsive to the families’ priorities. These providers can offer cultural continuity that can strengthen cultural identity and child-parent relationship. Parents and providers can work together on curriculum and values whereas language barriers make it difficult for parents to connect with more formal childcare programs.
Many immigrant parents believe that FFN care provides more personal attention for their children. Indeed, research shows that FNN providers often have low adult-child ratios, suggesting that these providers are able to spend more individual, quality time with each child. Although studies show that overall, the quality of FFN care is suboptimal to licensed programs, researchers are wrestling with appropriate assessment tools for FFN providers. The studies that show that center-based care predicts higher levels of cognition for children ages zero to three in the United States does not necessarily demonstrate that informal care cannot produce the same results. The potential of FFN care has yet to be measured due to its invisibility, diverse forms, and lack of financial and institutional support.
What is certain is that many families, especially immigrants, will continue to prefer FFN care and the early education and care workforce requires FFN providers to fulfill the demand for childcare. Increasing legislative and financial investments in FFN caregivers promote equity for immigrant families; it supports these workers, enhances the quality of care, and lessens the overburdened care industry. Offering immigrant parents and their informal childcare providers additional resources, including training, technical assistance, and access to subsidies, is critical in order to enhance access and improve child development outcomes.
Half of all immigrant caregivers in the early education workforce are providing private home or family-based care. A quarter of family-based providers in the United States identify as Latinx. Because childcare programs and resources are generally focused primarily or solely on licensed providers and are often limited or unavailable for FFN (license-exempt) providers, the majority of FFN providers earn on average merely $7,420 a year because parents and guardians are the only sources of payment. Even prior to the pandemic, nearly 22 percent of immigrant ECEC providers were living in poverty. This lack of appreciation or fair compensation is part of a broader, historical trend wherein work done by women of color within private homes is not recognized as “real” work either by the public or policymakers.
The Child Care and Development Block Grant biennial state plans found that only three states report that they have policies in place to make their childcare licensing regulations more accessible to providers from language minority or immigrant communities. Moreover, many immigrant FFN providers are not culturally connected and know that these subsidies are available. Spanish-speaking FFN care workers were half as likely to access subsidies as their English-speaking peers. Some states, including Florida and North Carolina, prohibit unauthorized immigrants from collecting any subsidies. Unsurprisingly, only 38 percent indicated that they received subsidies or other financial support other than payments from parents, compared to 74 percent of English-speaking FFN providers. Most states allow unlicensed childcare providers to receive subsidy payments, but a report in January from Home Grown found that the accessibility and amount of funding unlicensed providers get varies. Most states require household-wide background checks to receive payments, which experts say can make it less likely that undocumented providers or providers in mixed-status households will apply for assistance.
Immigrant providers, specifically, are often discouraged from becoming licensed due to costs, language barriers, and real or perceived barriers related to their immigration status. Expensive and onerous requirements dissuade care providers from applying for a childcare license. There needs to be a concerted effort to reduce legislative and administrative barriers to support immigrant FFN care providers. This can look like simplifying application processes, translation in multiple languages, revision of documentation requirements, and community outreach—the same mentioned recommendations for all public programs to reach immigrant families.
Yet another solution is creating funding avenues for FFN providers without requiring license. The Child Tax Credit provides flexibility for parents to use money how they want, trusting parents to find the best care for their children based on their specific needs, which might include linguistic and cultural continuity. Disability and elderly care can provide a sustainable model of family members receiving government payments to do care work.
Training and funding for FFN providers chosen and trusted by immigrant parents can be a way to promote culturally inclusive early education and care for their children. Some states have initiated training for refugee parents to become childcare providers, promoting additional income for refugee families and culturally competent environments. States can support providers who care for children who are linguistically diverse by offering financial incentives. California, for example, pays providers who care for dual language children at an adjusted childcare subsidy payment rate that is 10 percent higher than the state standard reimbursement for contracted providers.
States need to provide dedicated funding directly to providers and community-based organizations that work with FFN and immigrant providers. For example, in 2021, Minnesota Department of Human Services directed $1 million of the $48 million in federal CARES Act funding to state and local agencies working with FFN providers. $800,000 of the million went to four existing department grantees serving FFN providers across the state, with a focus on the Somali, Latinx, American Indian, and immigrant communities. The remaining money was distributed to small agencies, which must be at least 51 percent owned by a woman, racial minority, or person with a substantial physical disability.
FFN support programs can collaborate with trusted community organizations to personalize outreach at strategic locations, word of mouth, and going door-to-door. Training for immigrant FFN care supporters should be trauma-informed. Immigrant FFN providers carry many stressors: family-related stress, financial burdens, immigration-related stress, burnout, primary and secondary trauma, limited developmental knowledge and child rearing strategies, depression, anxiety, and social isolation. The caregivers’ wellbeing is inextricably and intimately connected to the mental health of the young child, impacting the children’s long-term achievement. The Pamoja Early Childhood Education Workforce Program in Colorado, for example, offers immigrant mothers a trauma-resilient training in several languages to do home visits with people who are already or interested in becoming FFN providers. With a grant from the Colorado Health Foundation, the co-organizer Lauren Dorn names FFN care as a “form of healthcare, … where the children are getting their brain growth, all of their positive, emotional, shared connections.” This program intervenes in the caregivers’ trauma and positions immigrant women in the role of teaching each other. In addition to advancing kin care, Pamoja offers a community to immigrant women, who are often isolated in their homes.
Innovative partnerships with Head Start and university groups allow immigrant families to tap into established and funded resources that can readily be tailored to respond to their specific needs. Another way to help support immigrant providers is to develop community networks for FFN providers through gatherings at local parks or community centers to share information and ideas. All Our Kin, a nonprofit group advocating for family childcare providers in Connecticut and New York, helps Spanish-speaking FFNs navigate the licensing process and helps FFN providers who aren’t looking for licenses to get access to other resources. Additionally, give immigrants a seat at the table to seek input from them in developing childcare policies and programs.