Table of Contents
- Checklist
- Introduction
- Household Economy
- Community Resilience
- A Pandemic of Racism
- Election Integrity
- Healthcare Surge Capacity
- Supply Chain Management
- Universal Access to Digital Services
- Banking and Payment Systems
- Economic Resilience
- Future of Work
- Epidemiological Readiness
- Porous Lines of Defense
- Institutions
- Policy Considerations
Healthcare Surge Capacity
No matter the cause of a mass casualty event, whether it was triggered by a foreign or domestic terrorist attack, a mass shooting, natural disaster, or pandemic, the ability of the healthcare system to address a surge is critical to building resilience. This is true for localized events, as much as it has proven true nationally, as COVID-19 hotspots shifted across the country, affecting cities, communities, and hospital systems with a moving wave of patients.
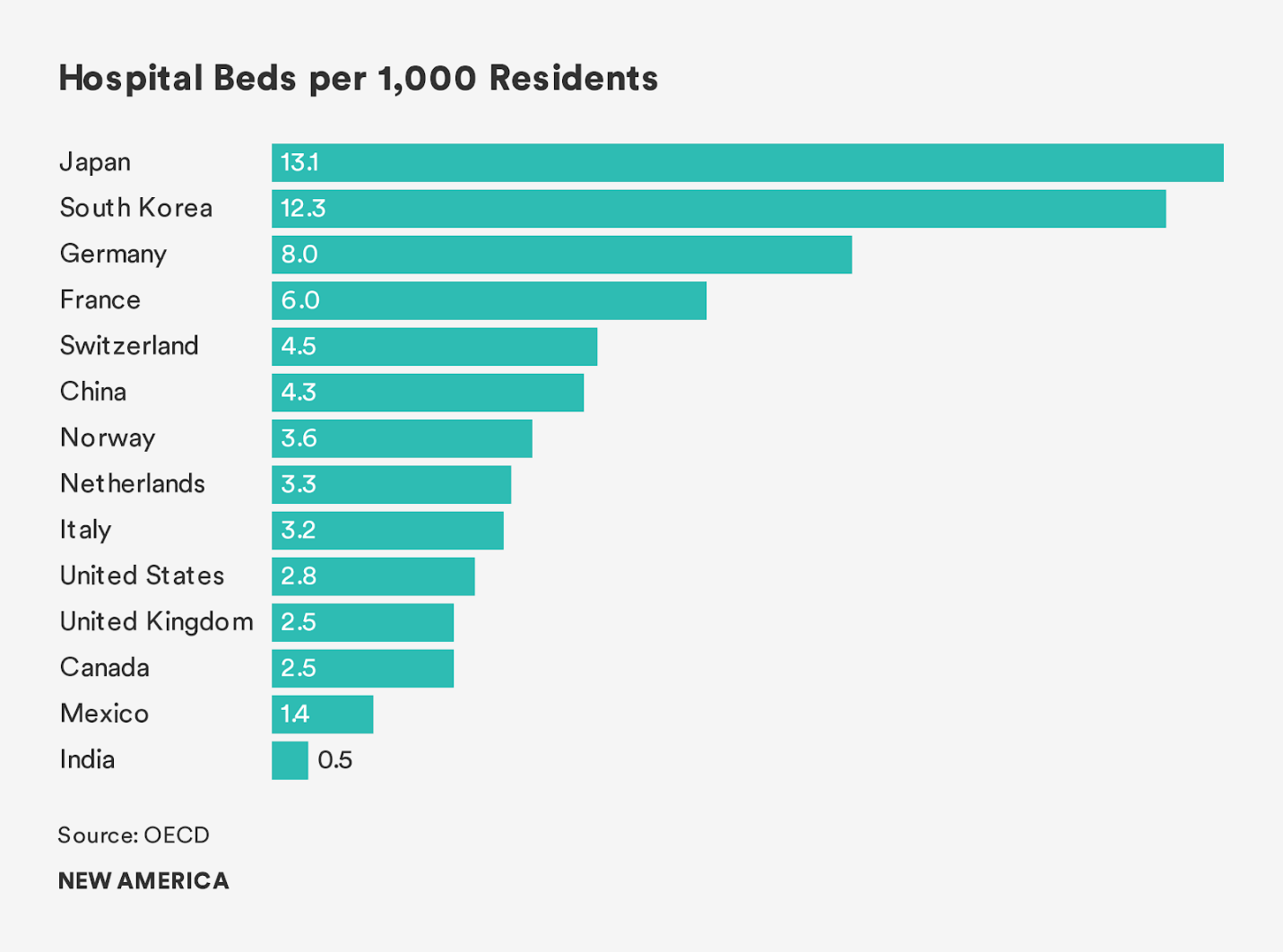
In the ranking of hospital beds per capita, a blunt measure of hospital surge capacity, the United States has 2.8 hospital beds per every 1,000 people in the country. This linear measure, while crude since it does not count other key ingredients of world-class healthcare such as trained medical professionals and the availability of necessary medical equipment, offers a good proxy for mass casualty readiness. By contrast, South Korea, which has fared well in the pandemic, has 12 hospital beds per 1,000 people and universal access to healthcare coverage. They deployed a rapid testing and contact tracing regime that served like a dragnet in containing the spread of COVID-19.
Increasing healthcare capacity at the physical and human capital levels is necessary as a post-pandemic area for improvement. While some healthcare systems performed better than others across the country, typically skewing to wealthier communities, the national health emergency scorecard did not get good grades. Indeed, much of the logistics and supply chain support called upon from the Federal Government and agencies like the Federal Emergency Management Agency (FEMA) required the mobilization of field hospitals and navy hospital ships, United States Naval Ship (USNS) Mercy and USNS Comfort to Los Angeles and New York City respectively—although neither was used to full capacity.
The shortfall in terms of medical surge capacity had less to do with hospital beds (especially as cities converted convention centers into field hospitals) and more to do with staff shortages and key materiel, including and especially PPE, ventilators, and other necessary equipment for the frontlines. Using the word strategic to describe the inventory in the national strategic stockpile of essential medical equipment to respond to a large-scale outbreak misses the mark. Indeed, as states and cities fought over supplies, sparking a bidding war and supply chain nightmare, stockpiles were quickly depleted. How public and private sector supply chains fared in this crisis and how to bring nearer to shore or on shore the industrial capabilities necessary to respond to future emergencies is an area for further review.
In terms of the human toll of the pandemic, at the time of publication more than 6 million confirmed cases were identified in the United States, and more than 180,000 people lost their lives. The real numerator and denominator of affected populations is not really known and likely numbers in the millions if antibody tests offer any guide. The frontline medical force serving as the human wall to contain the pandemic was stretched to the brink and are in every way the heroes of these dark times. In the worst hit hospital systems, such as in Manhattan, medical professionals resorted to creating their own makeshift PPE using garbage bags and other ill-suited materials due to supply shortages.
This was tantamount to sending soldiers to battle without body armor, helmets, or ammunition. Needless to say, medical readiness against future pandemics or other mass casualty events needs to be prioritized, as much as universal access to the healthcare system needs to be made available to citizens irrespective of their insured status ahead of the next public health emergency.
The medical frontlines were also strained by the fact that for 13.8 percent of the working age adults who are uninsured (notwithstanding the fact that relief bills called for the removal of COVID-19 testing costs) faced a double-jeopardy. On the one hand, the costs of treatment would be a burden, as much as not getting treated or screened for the virus would potentially endanger others, contributing to the vicious cycle of cases. Indeed, many countries around the world called up retired medical professionals and accelerated the frontline deployment of medical professionals in training like so many reservists in past wars. A veritable medical draft occurred around the world and in parts of the United States in order to buttress frontline capabilities to deal with patient loads. To them, the almost certain prospect of a second wave in the fall is an ill-portent of the long road ahead to push this latest coronavirus back to the shadows from whence it came.
The economic cost of flattening the curve of cases, which were hampered by the general lack of testing at a national scale, along with a shortage of necessary testing equipment like nasopharyngeal swabs, was an indictment of U.S. industrial capacity. This shortfall caused many to invoke the need for war powers to be exercised to compel the private sector to divert their supply chains and production capacity to manufacture necessary medical equipment. Private industry responded to these calls, some begrudgingly under the threat or limited use of war powers, others on their own volition.