
Providing Care Changes Men
Table of Contents
- Executive Summary
- Introduction
- I. Providing Care Can Shape Men’s Attitudes and Beliefs
- II. Men Who Care
- III. Men and Work-Family Conflict: The Heavy Toll on Men who are High-Intensity Caregivers and/or Parents
- IV. An Overwhelming Majority of Men Value Care and Believe it Should be Equally Shared. But Belief Isn’t Associated with Practice.
- Conclusion
- Methodology
Abstract
This report seeks to better understand men who give care—who they are, what they do, and how they think. This was done by comparing the experiences of men who have ever provided care—whether to adults, children, or children with a medical, behavioral, or other condition or disability—with men who have not. We initially sought to explore a central question: whether men’s experience of providing care influenced their attitudes about the value of care. We were curious to explore whether men valuing care would be associated with them doing more of it.
It’s a critical question. Men say they want to share care work equally with their partners. But they don’t. Understanding what stops men from taking on more care responsibilities, and, when they do, what encourages them to continue, is key to creating not only more gender equity, but better health and wellbeing for men, women, children, and families.
In a nationally-representative survey of 2,966 American adults, conducted in partnership with NORC at the University of Chicago and five online focus group discussions using 20|20 Research’s QualBoard facilitation platform collected before the outbreak of the COVID-19 global pandemic, we found that men in general, regardless of their care experience, overwhelmingly say they do value care, with large majorities saying the unpaid care work of home is just as important as paid work. We found, as other surveys have, that large majorities of men say that men should share care work equally with women. And yet we found that men’s belief in gender equality and the value of care did not necessarily translate into men taking on more care responsibilities. In fact, there is a substantial disconnect between what men say is ideal when it comes to sharing care work, and what they actually do.
Acknowledgments
This study was conducted with support from the Robert Wood Johnson Foundation and Pivotal Ventures, an investment and incubation company created by Melinda Gates. The author wishes to thank the men from all walks of life who generously agreed to share their stories and perspectives in the survey, focus groups, and extensive interviews, and to the men who gave our team guidance on shaping the focus group questions. Thanks also to NORC for their thoughtful and rigorous work and to the reviewers who took time out of their busy schedules to share their insights and expertise, Caitlyn Collins, Dan Carlson, Jessica Calarco, and Leah Ruppanner. Special thanks to reviewer Ken Matos, who helped spark the idea for this project over lunch at a Work Family Researchers Network conference. Special thanks also to the dedicated work of Melissa Saphir, my guardian angel of data analysis, who helped me see through the weeds and kept me rigorous and honest. Thanks, too, to Better Life Lab senior fellow Vicki Shabo, for her thoughtful review, and to the many valuable contributions of the Better Life Lab team—Haley Swenson, Sade Bruce, Roselyn Miller, Jahdziah St. Julien, Emily Hallgren, and Stavroula Pabst. And to former colleagues Amanda Lenhart, who spearheaded much of the data gathering work, Alieza Durana, Elizabeth Weingarten, and Leah Crowder. And to the always-creative and patient New America Communications team.
Executive Summary
We set out in this report to better understand men who give care—who they are, what they do, and how they think. We did so by comparing the experiences of men who have ever provided care—whether to adults, children, or children with a medical, behavioral, or other condition or disability—with men who have not. We initially sought to explore a central question: whether men’s experience of providing care influenced their attitudes about the value of care. We were curious to explore whether men valuing care would be associated with them doing more of it.
It’s a critical question. Men say they want to share care work equally with their partners. But they don’t. Understanding what stops men from taking on more care responsibilities, and, when they do, what encourages them to continue, is key to creating not only more gender equity, but better health and wellbeing for men, women, children, and families.
In a nationally-representative survey of 2,966 American adults, conducted in partnership with NORC at the University of Chicago and five online focus group discussions using 20|20 Research’s QualBoard facilitation platform collected before the outbreak of the COVID-19 global pandemic, we found that men in general, regardless of their care experience, overwhelmingly say they do value care, with large majorities saying the unpaid care work of home is just as important as paid work. We found, as other surveys have, that large majorities of men say that men should share care work equally with women. And yet we found that men’s belief in gender equality and the value of care did not necessarily translate into men taking on more care responsibilities. In fact, there is a substantial disconnect between what men say is ideal when it comes to sharing care work, and what they actually do.
Instead, what became clear, particularly in analyzing the focus group discussions and in journalistic interviews conducted with a variety of men to capture men’s experience providing care during the pandemic, is that the experience itself of providing care is key. These conversations, in addition to the survey data, suggest that the experience of providing care is what can shape men’s attitudes about care or transform men’s lives.
The notion that men’s experience providing care can shape attitudes, beliefs, and behaviors was most apparent in our focus group discussions. Men who had experience providing care were much more likely than men in the general population group to say that men, not just women, have a natural instinct to care, that providing care is a skill that can be learned, and that society’s expectations and workplace structures are often what keep men from giving care. These conversations showed that it is far easier for men to express a belief that care should be equally shared and much more difficult for men to act on that belief. Further, men who’ve experienced caring for another showed a much more complex and nuanced view of care itself. We asked participants in two focus groups of men to provide images of a “caregiver.” Nearly all the men in the general population group offered photos of female nurses or female uniformed home health aides in medical settings or with the elderly with walkers or wheelchairs. Yet men in the group who had experience caring for an adult, in sharp contrast, shared personal photos of themselves, their children and families, or intimate images of hands clasped or an embrace. In other words, men without the experience of directly providing care immediately associated care with women. And those who had provided care immediately saw themselves.
Terminology
High-Intensity Caregivers and/or Parents: In analyzing our survey data, we initially planned to analyze and compare the experiences of three groups of men: men who care for adults, fathers, and men who are not caregivers. However, it quickly became clear that a significant number of respondents have both provided care for an adult family member or close friend, and are, at the same time, parents who have cared for a child under 18 with a medical or behavioral condition or disability (special needs.) In our survey, 60 percent of parents who have cared for children with special needs have also cared for an adult. Conversely, nearly one-third of those who have cared for an adult are also parents who have cared for children with special needs. And across 27 comparisons, we found only three statistically significant differences in attitudes between those who care for adults, parents who care for children with special needs, and those who fall into both categories. For these reasons—because there is so much overlap in actual people and because of the similarities in attitudes—we chose to group these adults together as High-Intensity Caregivers and/or Parents, abbreviated in this report as HICP.
We compared the experiences and attitudes of those in the HICP group to parents who have never cared for a child with special needs, a group we labeled Other Parents (or Other Fathers, when discussing men exclusively.) We compared both of these groups of caregiving adults with those who have never provided care, i.e. Non-Caregivers. To increase our understanding of men’s experiences with caregiving, some of our analyses compared these three groups while looking only at men, while for other questions, we compared men in the HICP or Other Parent group to women in these groups.
Caregiving: The word “caregiving” means different things to different people, and even is defined differently in national surveys conducted by different organizations. For some, it encompasses a wide variety of caring activities—parenting, caring for an adult, self-care, paid and unpaid care work—on behalf of a variety of people. Others define the word narrowly. For instance, federal legislation and some advocacy organizations refer to “family caregivers” as adult family members or others and who provide ongoing assistance to people with a “chronic or other health condition, disability, or functional limitation.” For the purposes of this report, we use the term “caregiving” to refer to a broad range of care tasks and responsibilities, including hands-on and hands-off care and parenting. Thus, we also refer to two of our three groups—the HICP and Other Parent groups—as “caregiver” groups, because individuals in both these groups perform the broad range of care tasks and responsibilities that we consider to be caregiving.
In exploring men’s experience with care, a central question remains—what keeps men from doing a more equal share of the care work in the United States that they say they say is their ideal? We found evidence that traditional gendered expectations do play a role. But those are shaped and reinforced by inflexible and demanding work cultures, financial pressures, a lack of family-supportive public policies, and cultural expectations about who should or is best suitable for caring. Together, these forces keep men from having the often transformative experience of providing care, and from sharing care responsibilities equally.
Although the data was collected before the global pandemic, it can serve as both a baseline to measure change as well as a useful guide in better understanding men’s experience providing care, the channels that enable them to do it, and the barriers that keep them from it, how it transforms them, and the lasting impact men’s caregiving may have in the future.
Key Findings
The experience of providing care can shape men’s views about care. We asked participants in two focus groups of men to provide images of a “caregiver.” Nearly all the men in the general population group offered photos of female nurses or female uniformed home health aides in medical settings or with the elderly with walkers or wheelchairs. Men in the group who had experience caring for an adult, in sharp contrast, shared personal photos of themselves, their children and families, or intimate images of hands clasped or an embrace.
A Caring Nation
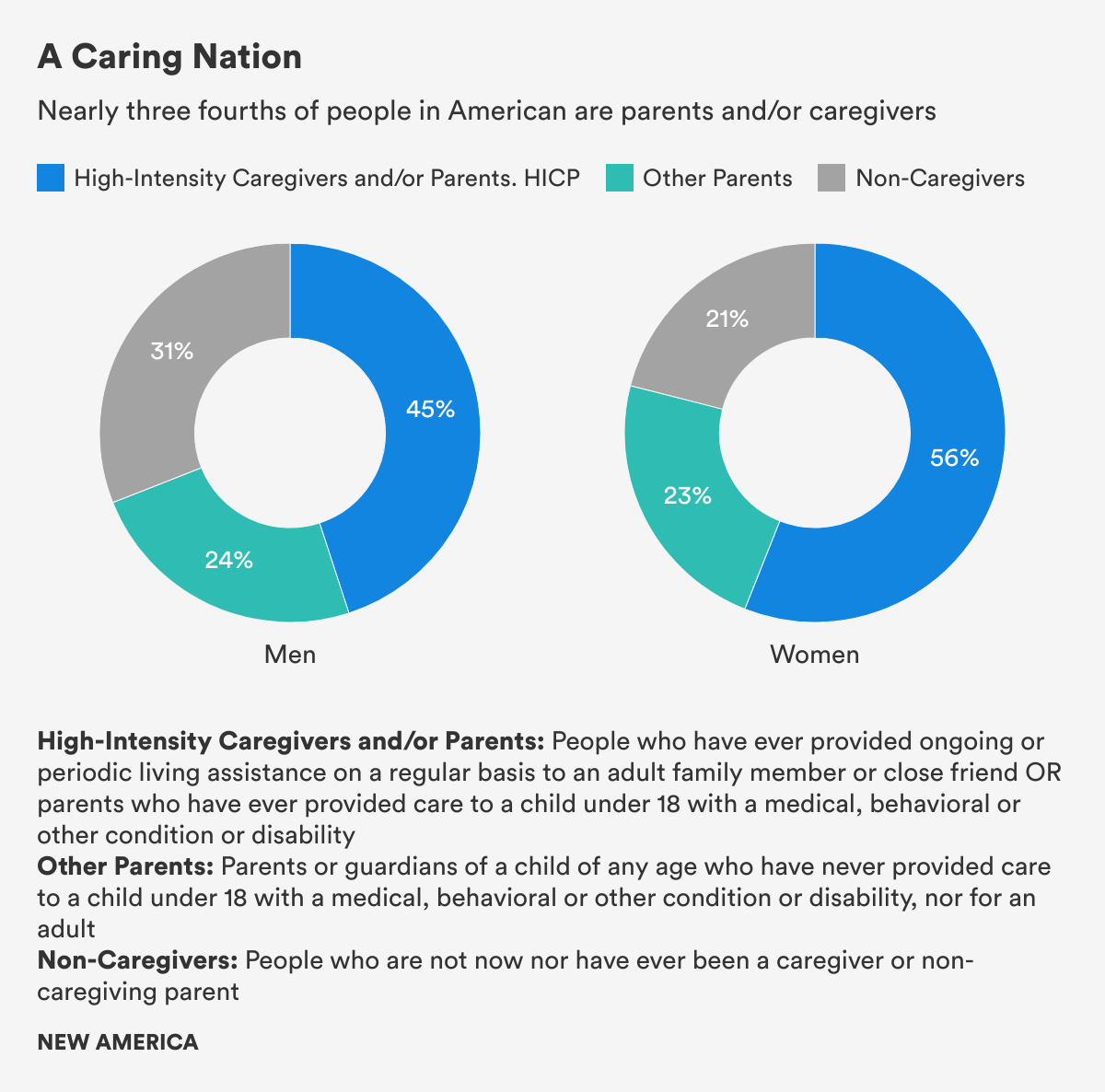
- Nearly three-fourths of all survey respondents are High-Intensity Caregivers and/or Parents, HICP, who have ever provided care to an adult or child under 18 with a medical, behavioral, or other condition or disability (special needs) or Other Parents of children without special needs.
- Although more women fell into the High-Intensity Caregiving and/or Parenting group (56 percent), more than four in 10 men (45 percent) said they, too, have provided this labor-intensive and often invisible care for adults or children with special needs at some point in their lives as well.
Men Value Care and Want to Share Care Work Equally
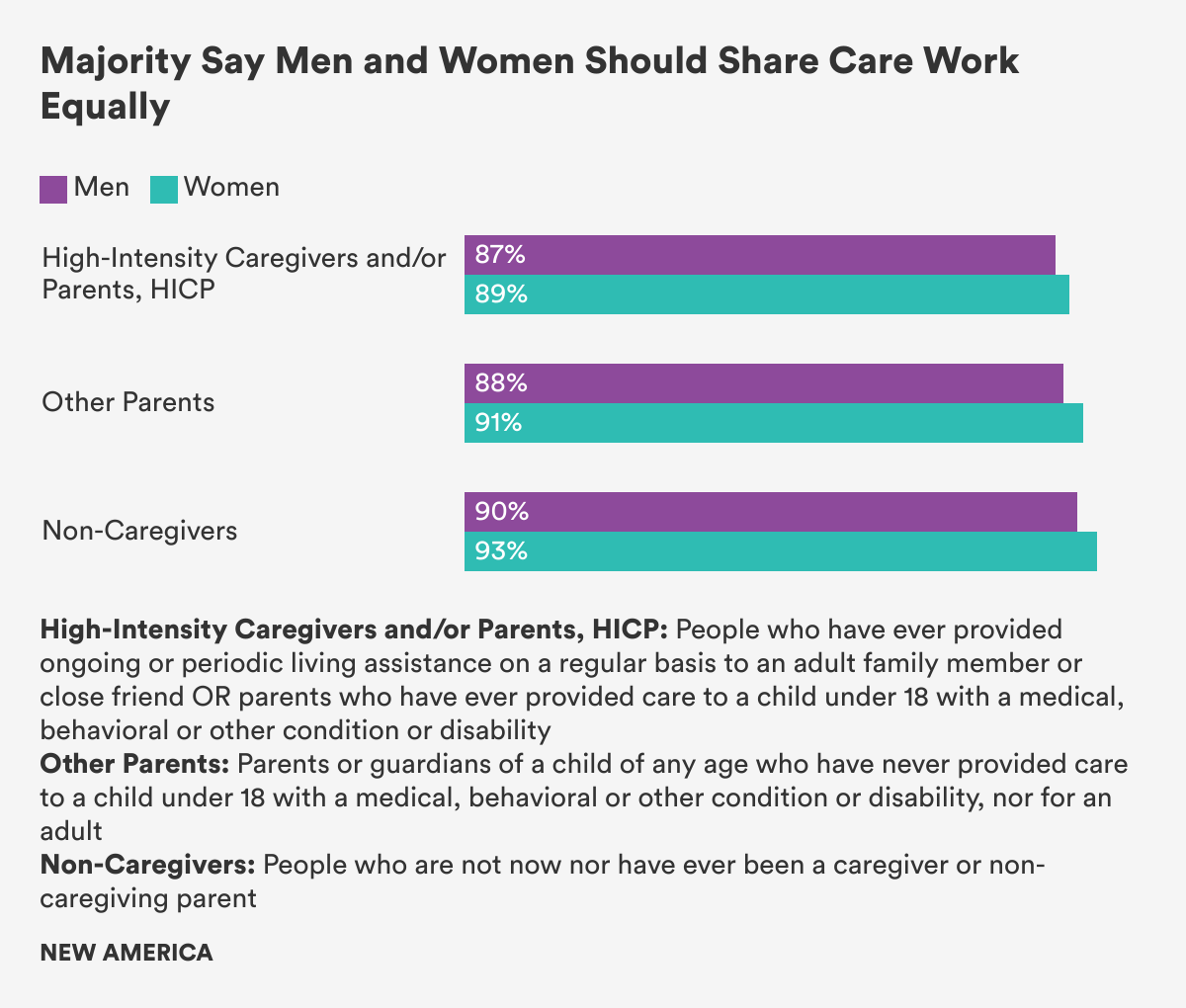
- Overwhelming majorities of men—more than 80 percent—regardless of their experience providing care or not, believed that unpaid care work at home is as valuable as paid work, valuable to society, and that men and women should share care responsibilities equally.
- The gap between the ideal and actual behavior is large: 91 percent of all survey respondents said care work should be equally shared between men and women. Yet 45 percent said that caring responsibilities fall primarily on women, (46 percent said the care was shared equally. Just 4 percent said caring responsibilities fall primarily on men.)
Men and Women Differ on How Much Men Provide Care
- Men were nearly twice as likely as women (60 percent vs. 32 percent) to say that the division of care labor is equitable when a family member has a serious illness, or a disability, or needs extra help as they get older.
- Roughly one-third of men who are High-Intensity Caregivers and/or Parents, HICP, and Other Fathers said they lived in families where men do the majority of care work at home. Fewer HICP women and Other Mothers, roughly one in five, said the same.
Men who are High-Intensity Caregivers and/or Parents Carry a Heavy Load
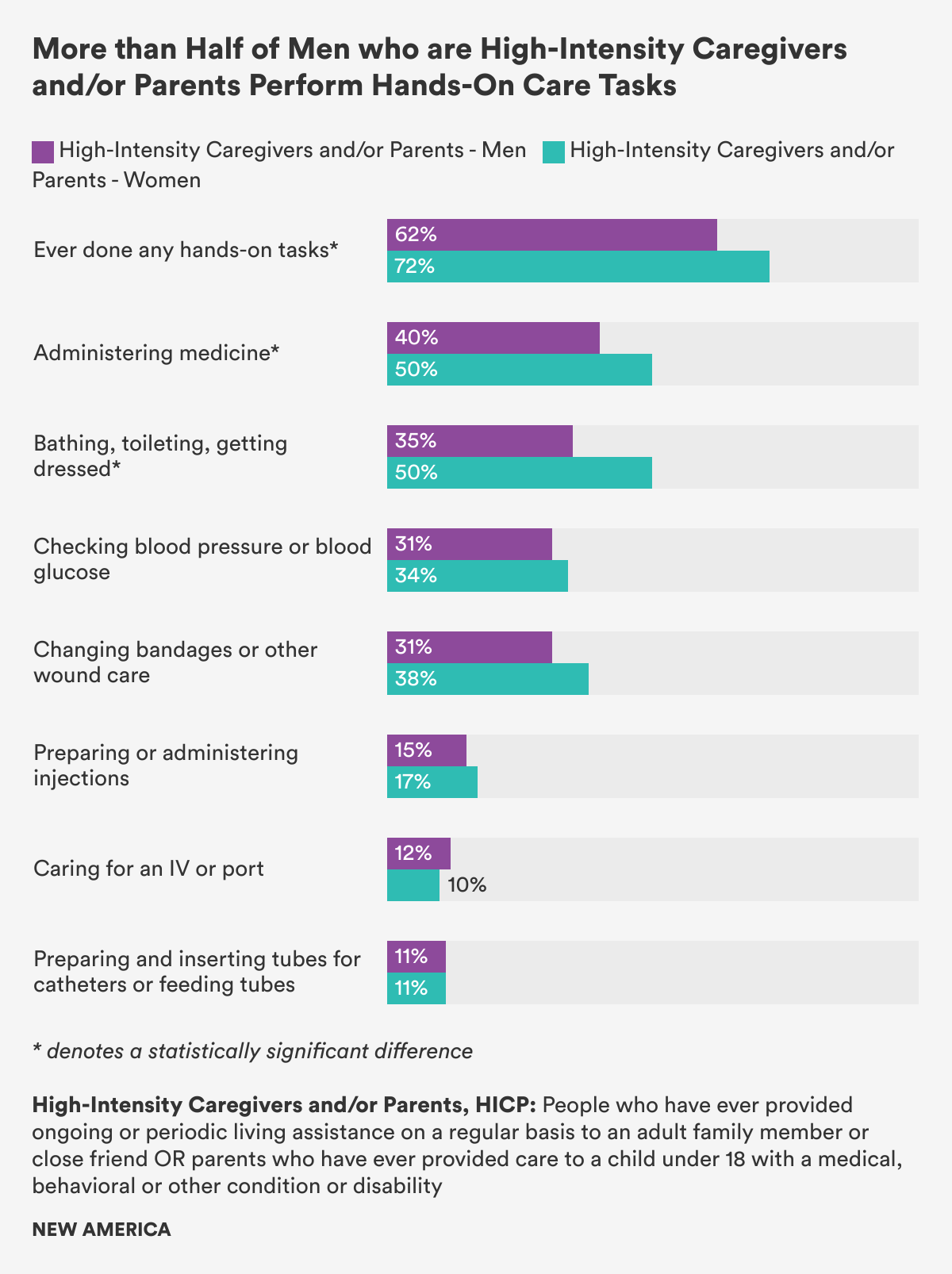
- Men who care for adults or fathers of children with special needs perform many of the same care tasks that women with the same care responsibilities do, with six in 10 HICP men performing the intimate hands-on tasks more often associated with women, like administering medicine, bathing, toileting, getting dressed, and changing bandages.
Men who Provide Care Face Work-Life Conflict and Burn Out
- Men who are High-Intensity Caregivers and/or Parents, HICP, experience more work-life conflict than Other Fathers and men who are Non-Caregivers—41 percent of HICP men said they had to put off work because of the demands on their time at home, compared to 33 percent of Other Fathers and just 10 percent of men who are Non-Caregivers.
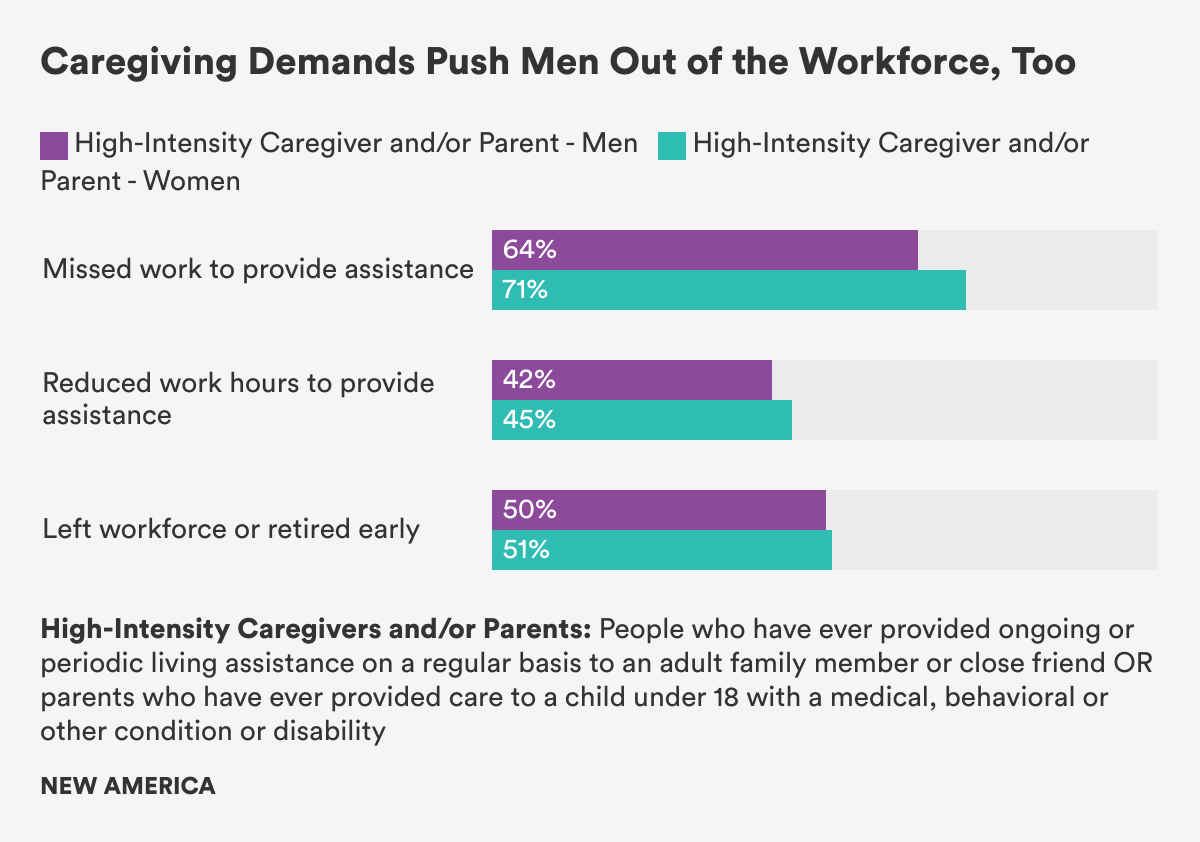
- More than two-thirds of employed men who are High-Intensity Caregivers and/or Parents, HICP, reported missing work, reducing work hours, or leaving the workforce entirely because of care duties, similar to the shares of HICP women.
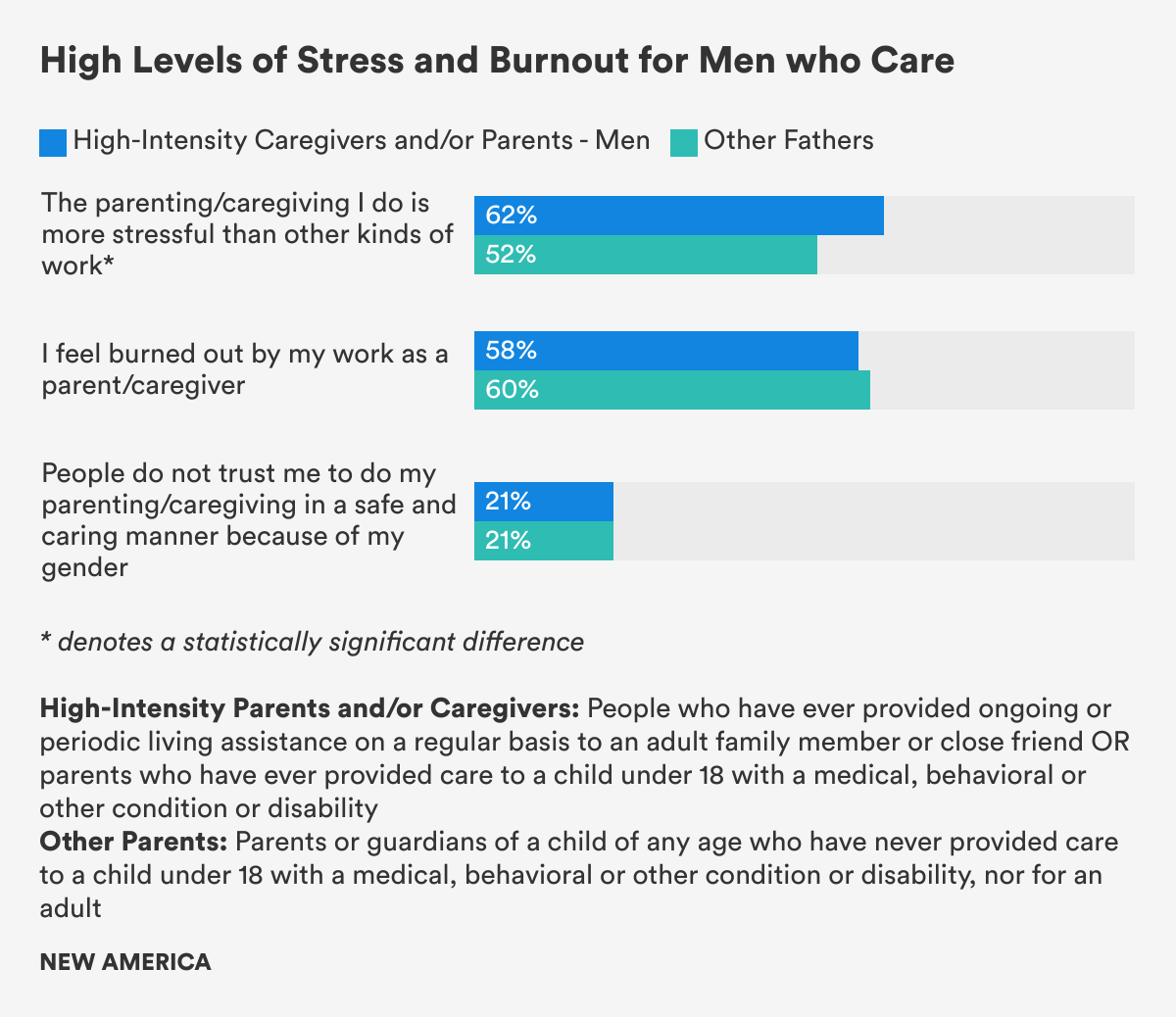
- Regardless of gender, six in 10 caregivers—both High-Intensity Caregivers and/or Parents and Other Parents—reported feeling burned out by their care responsibilities.
Men Anticipate Needing Time Off Work to Care
- Large shares of people in all groups anticipate needing time off work to give care in the future, including nearly half, 47 percent, of Non-Caregivers.
Men who Care Face Mistrust and Stigma
- One in five caregiving men, both High-Intensity Caregivers and/or Parents and Other Fathers, said that people do not trust them to give care or to parent in a safe and caring manner because of their gender.
Introduction
I hear and I forget
I see and I remember
I do and I understand
– Confucius
When the COVID-19 pandemic forced his workplace to shut down and his managers to lay him and other staff off in March 2020, Ronald Taylor, an occupational therapist in Portland, Ore., became the primary carer for his two daughters, ages 5 and 8, whose schools had also shut down. His wife, Kerala, a marketing and strategic planner, was able to work remotely and keep the family afloat financially. For weeks, Ronald was with his children 10 hours a day, 7 days a week and in charge of the home front.
While some men in similar situations—during the pandemic and in the Great Recession of 2008—may have felt out of their depth, for Taylor, “it was wonderful in many ways.” But that’s because the experience of hands-on care was not new. When his eldest daughter was born, he stayed home caring for her for 15 months because his wife earned more money and the couple couldn’t afford childcare if they both worked. “It changed me as a person,” he said.
Taylor was a paramedic for six years. He has a graduate degree. He’s the only Black male hand therapist in the state of Oregon. “And the hardest job I’ve ever had was taking care of my baby daughter for 10 hours a day,” he said. “Most men don’t have any idea what that’s like, or what their wives are going through. They think, ‘I went to work, I worked hard.’ I want to tell them, ‘Yeah, she worked harder.’ And unless you have that experience, you think paid work is more important than taking care of another human being.”
Taylor remembers taking his baby daughter out in her stroller one day. He walked by a construction site. “I just felt so ridiculous,” he said. “I’m supposed to be a man, and I’m pushing this baby stroller while my wife works. This one guy asked me, ‘Oh, you’re just taking care of your baby, huh?’ I said, ‘Yeah, but I wish I was doing what you’re doing.’ And then the guy said, ‘I wish I was doing what you’re doing.’”
As he reflected on this pivotal moment in his life, Taylor paused. “I think if we could do it more, and it was respected in society, I think a lot more men would like to be around their kids more,” he said. “But I don’t think it’s something society values.”
In 2020, an unprecedented pandemic has upended daily life around the globe. Never before has the central role that care plays in our lives been made more clear as families struggle with work and care responsibilities in the face of school closures and childcare shutdowns while contending with the needs of isolated and aging parents, illness, fear, and even death.
Women and mothers, who are still culturally expected to be primary carers, typically spent about twice the amount of time giving care before the pandemic. During the upheaval, as schools and childcare facilities have shut down or reduced in-person attendance, women have taken on the bulk of the expanded load of care work and homeschooling and are paying the price—cutting back on work hours or dropping out of the workforce entirely at higher rates than men, and experiencing high rates of stress, anxiety, and sleeplessness. Some academics and advocates worry women will be set back a generation.
… women have taken on the bulk of the expanded load of care work and home schooling, and are paying the price.
Yet, in a phenomenon that bears close attention, the lives of men like Taylor have also changed dramatically. Nearly overnight, an enormous number of white-collar men who were accustomed to being rewarded for working long hours in offices, often reached after lengthy commutes, began working remotely. In-home offices, at kitchen tables, in laundry rooms, and many with children underfoot. More than three-quarters of essential healthcare workers are women. They’ve been forced to work long hours in the pandemic and are simply unable to be the primary carers at home. It remains to be seen whether their male partners will have been forced to step up and take on more care responsibilities. (One study using survey and interview data with mothers of young children in the early weeks of the pandemic found that some front-line health workers relied on extended family stepping in to help with childcare rather than on their spouse or partner.)
Unemployment and furloughs have been more severe for women and women of color in this pandemic because they’re overrepresented in the service and hospitality industries that have been hit hardest. But millions of men have also lost jobs and livelihoods—more than 20 million people in the United States were unemployed in May 2020 at the height of the pandemic-related shutdowns, and 11 million people remained out of work in October 2020—disrupting gendered patterns of work and care. Research conducted at the height of the first wave of the pandemic found that while women were doing more care work and homeschooling than men, men were still doing far more care work than they had before the pandemic, leading, in some families, to more equal sharing of care and domestic labor.
So the question is: will the experience of doing more hands-on care—or, at a minimum, the day-to-day exposure to just how much work it takes to give care and run a household—change men’s attitudes, beliefs, and behaviors? Will men, for so long defined by the gendered expectation of being primary breadwinners and a family’s financial provider, remain more active carers once the pandemic ends? Will they, like Taylor, become changed by this experience of care? And will that lead to healthier children and families, as research suggests, and to fairer divisions of work and care that could finally push forward the journey toward gender equality that’s been stalled for decades?
Will men, for so long defined by the gendered expectation of being primary breadwinners and a family’s financial provider, remain more active carers once the pandemic ends?
Previous studies on whether men’s experience of providing care changes their attitudes and behaviors are mixed. Some have found that men’s involvement in household labor is often “situational,” meaning they’ll pitch in or take over when they have no other choice. For instance, men whose wives work opposite schedules from them or who work evening shifts and are home with the kids during the day tend to do more at home, whether they believe in gender equality or not. It’s just what they have to do—a phenomenon that lawyer and work-life scholar Joan C. Williams describes as blue-collar men and fathers “walking the walk” of gender equality, even if they don’t talk the talk. For white-collar men, it’s often the opposite, she found—they say they believe in gender equality, though they’re in more traditional partnerships and divisions of labor, largely because of the expectation of long work hours for white-collar jobs. And men in heterosexual couples who telecommuted before the pandemic tended to pitch in more with child care and housework only if their partner or spouse worked full-time.
Yet when men lost jobs in the Great Recession of 2008 and took on more household and care work at home, researchers found that many began to move away from the breadwinner identity to find meaning as active, engaged fathers.
Throughout much of the twentieth century, academics all but ignored men as carers, seeing their role in the home as “irrelevant.” Even when women began entering the workforce en masse in the 1970s, change has been slow in the cultural expectation that care work is “women’s work.” Not long after Wade Horn, assistant secretary for children and families at the Department of Health and Human Services under President George H.W. Bush, said that men being involved in care work was “nonsense,” sociologist Scott Coltrane released a groundbreaking qualitative study on men and care. He reported that men were “transformed” by their experience of care work, with fathers developing increased sensitivity to their children, their families, and the difficult, time consuming, and yet profoundly meaningful work of care and connection. In other research, fathers of children with special needs have reported that their experiences providing care increased their patience, empathy, tenderness, and humility.
Already, intriguing research is emerging about how men’s roles in care work are evolving during the pandemic. One survey of Australian families under lockdown in May 2020 found that, with schools and childcare closed, the domestic load of unpaid work rose for both men and women, though women took on a greater share of the responsibility. Still, men began spending about as much time providing care during the pandemic as women had pre-pandemic, narrowing the relative gender gap in time spent on childcare from 52 percent to 41 percent. Another study, based on a U.S. sample, similarly found that 10 to 15 percent of the different-sex couples studied had moved toward a more equal division of unpaid caring and housework in the pandemic.
Our quantitative survey sheds important new light on who men who give care are and shows how much they do, how they, too, struggle with work-family conflict, and that men who are High-Intensity Caregivers and/or Parents, HICP, have been forced to reduce hours or drop out of the workforce at rates similar to HICP women. And the perspectives shared in our qualitative research, in addition to previous research, suggest that men’s lives can be profoundly transformed by the experience of giving care. The men in our focus group discussions repeatedly said that while care work can be exhausting, emotionally draining, stressful, and lead to burnout, it is also deeply meaningful. Their names have been changed to protect their identities, except in cases where they’ve permitted us to use their identities and comments.
James, 49, from Florida, is one of our focus group members with experience caring for an adult. He cares for his mother, administering medicine, handling her finances, driving her to medical appointments, and doing all he can to keep her living independently at home and out of assisted living or a nursing home. “It is time consuming,” he told us. “But it is worth it.”
Indeed, research on men who’ve taken paid family leave to spend time caring for loved ones shows the experience can have deep, long-lasting impacts on the health and wellbeing of men and their relationships with their partners, their families, and their children. In many countries, men who’ve taken paid leave wind up becoming more engaged and active in their children’s lives over the long term. They even live longer. And yet one study in Spain found that men who took paid leave to care for an infant were less likely to want any more children. Possibly, the researchers surmised, “due to their increased awareness of the costs of child-rearing.”
When it comes to women in the workplace, there are rafts of research studies, surveys, employee resource groups, special programs, task force studies, recommendations, and self-help books. But we know very little about men and their experience as carers.
Building on the emerging work of academics, the Pew Research Center, Boston College Center for Work and Family, Promundo, and others, the Better Life Lab sought to help fill in some of the blanks on men and care with a nationally representative survey, in partnership with NORC at the University of Chicago, and a series of online focus groups and additional qualitative reporting. In this report, one in a series using our data on men and care, we provide a clearer picture of what we know about men who give care—who they are, what they do, and how they think about it. And we probe the question of how their exposure to giving care impacts their lives, attitudes, behaviors, and those around them.
Although the data was collected before the global pandemic, it can serve as both a baseline to measure change as well as a useful guide in understanding men’s experience providing care, the channels that enable them to do it, the barriers that keep them from it, and the lasting impact men’s caregiving may have in the future.
Terminology
High-Intensity Caregivers and/or Parents: In analyzing our survey data, we initially planned to analyze and compare the experiences of three groups of men: men who care for adults, fathers, and men who are not caregivers. However, it quickly became clear that a significant number of respondents have both provided care for an adult family member or close friend, and are, at the same time, parents who have cared for a child under 18 with a medical or behavioral condition or disability (special needs.) In our survey, 60 percent of parents who have cared for children with special needs have also cared for an adult. Conversely, nearly one-third of those who have cared for an adult are also parents who have cared for children with special needs. And across 27 comparisons, we found only three statistically significant differences in attitudes between those who care for adults, parents who care for children with special needs, and those who fall into both categories. For these reasons—because there is so much overlap in actual people and because of the similarities in attitudes—we chose to group these adults together as High-Intensity Caregivers and/or Parents, abbreviated in this report as HICP.
We compared the experiences and attitudes of those in the HICP group to parents who have never cared for a child with special needs, a group we labeled Other Parents (or Other Fathers, when discussing men exclusively.) We compared both of these groups of caregiving adults with those who have never provided care, a group we called Non-Caregivers. To increase our understanding of men’s experiences with caregiving, some of our analyses compared these three groups while looking only at men, while for other questions, we compared men in the HICP or Other Parent group to women in these groups.
Caregiving: The word “caregiving” means different things to different people, and even is defined differently in national surveys conducted by different organizations. For some, it encompasses a wide variety of caring activities—parenting, caring for an adult, self-care, paid and unpaid care work—on behalf of a variety of people. Others define the word narrowly. For instance, federal legislation and some advocacy organizations refer to “family caregivers” as adult family members or others and who provide ongoing assistance to people with a “chronic or other health condition, disability, or functional limitation.” For the purposes of this report, we use the term “caregiving” to refer to a broad range of care tasks and responsibilities, including hands-on and hands-off care and parenting. Thus, we also refer to two of our three groups—the HICP and Other Parent groups—as “caregiver” groups, because individuals in both these groups perform the broad range of care tasks and responsibilities that we consider to be caregiving.
Previous research has also found differences and “unique stressors” in the experience of fathers who have provided care to a child with special needs compared to fathers who have never cared for a child with special needs. About one in five children under 18 require special accommodations or services due to a chronic physical, developmental, behavioral, or emotional condition, and about two-thirds of these children require comprehensive services in addition to medication, according to the U.S. Department of Health and Human Services. These additional needs can be challenging, overwhelming, and stressful for parents. Research shows that in addition to higher levels of marital stress and lower relationship satisfaction, fathers of children with special needs experience greater child-related stress than other fathers. And because children with special needs can require specific routines or support structures, parents, and fathers in particular, may find it more difficult to manage care responsibilities with work demands.
We found that, even before COVID-19, men said they were doing much more care work than they are often given credit for—by their partners, families, their workplaces, by policymakers, in the national conversation, and even in their own minds. Though it’s important to note we asked about providing specific care tasks, not the frequency or duration of performing them, and that some studies have found men often think they’re doing a larger share of care work than women think they are. We found that some men’s limited view of what providing care means, in addition to the still-powerful biased traditional belief that men are suited to breadwinning and women to care work, are part of what keeps men from providing care. But those are not the only barriers. There are also structural, cultural, and financial obstacles that push men into breadwinning roles, making it far less likely and far more difficult for men to actively choose to provide care if they wish.
And, as other studies have, we found a wide gulf between what men say is ideal and what they actually do. For instance, 91 percent of our respondents said that care responsibilities should be equally shared between men and women, and men in all groups overwhelmingly said men and women should share care responsibilities equally. Yet when a family member is ill, has a disability, or needs long term care, 45 percent of our respondents said the responsibilities mainly fall on women. (46 percent said the responsibilities are divided about equally. Just 4 percent said they fall mainly on men.)
Figure 1
Often, we found men’s care work happens under the radar in a way that would hide their care in formal surveys or from public view. For instance, rather than use formal work-family supportive policies as many women do, many men were able to use the flexibility that comes from being in a position of power or privilege. George Smith, one of our focus group members who agreed to let us use his full name, is a financial planner, father of four, and primary carer for his ailing 77-year-old mother. Yet he’s never officially taken paid family leave for care, even when his mother was in the hospital for nearly two months. Instead, he uses paid sick and vacation time when he needs to and works a remote, flexible schedule in order to care for her. “I just incorporate it into my paid time,” he said.
Our initial question, as we began to analyze the survey data, was whether the experience of providing care would be associated with men valuing it more. Or conversely, if they believed care work was valuable, whether that belief would be associated with providing care. We didn’t find that. Instead, we found that men, by and large, say they do value care, whether or not they have ever provided care to loved ones. But that theoretical valuing of care doesn’t translate into their actually doing it. Rather, our focus groups and interviews suggest that when men actually do give care, the experience can be life-changing.
Men, by and large, say they do value care, whether or not they have ever provided care to loved ones… when men actually do give care, the experience can be life changing.
So the real question is, if men do value care, and express a preference for more equally sharing care responsibilities, what is keeping them from having that potentially transformative experience and being as engaged in care work as they would like? And what needs to change for that to happen? Our data suggest that transforming work culture, family-supportive policy, and gender norms to recognize that workers of all genders have care responsibilities is key to creating space for men to give care and to making the lasting social change that will increase equity and benefit the health and wellbeing of men, women, children, families, and ultimately all of the economy and society.
I. Providing Care Can Shape Men’s Attitudes and Beliefs
A Picture Paints a Thousand Words
The disconnect between what men say is ideal when it comes to equally sharing care and the reality of stark gender differences, before and during the pandemic, raises questions around whether that expressed egalitarian belief is superficial or said for public show. So, to better plumb the depths of what men really think about care work, their own internal and perhaps subconscious biases about who they think should be responsible for providing it, and how they see their role, we convened several focus groups. It became apparent analyzing the transcripts of these conversations that it is indeed far easier to espouse an egalitarian view—our survey data showed that men overwhelmingly say care work is as valuable as paid work and should be shared equally with women—than it is to act on that belief.
The conversations were utterly different between a group of men who had provided care for an adult and a general population group of adult men. The conversations can’t definitively prove that an experience of providing care caused a transformation of attitude, belief, or behavior. It is possible that these views and behaviors predated the caring experience. Yet the very different conversations in the two very different groups of men show that the experience of providing care is associated with a much more nuanced and personal view of care and providing care and strong beliefs that men are just as good at it, and that, regardless of gendered beliefs of who is “naturally” better at it, that caring is a skill that can be learned.
We asked men in two separate focus groups—one group of men who had cared for an adult, and another general population group of men who had not—to upload an image into an online discussion of what came to mind when they thought of the word “caregiving.”
In the 13-member general population group of men, all but one posted images of women. Two posted photos of mothers with newborns. And 10 posted images of female nurses or home health aides, and most of them in medical settings, wearing nursing scrubs or pushing an elderly person in a wheelchair, or giving medical care in a hospital or clinic.
Leonard, 42, from Dallas, like the majority of the men in the general population group, posted a photo of a professional female health worker. “I think of a middle-aged woman who is a nurse caring for an older man’s medical needs in assisted living or in his home. This is perhaps the first image that came to mind [because] my grandfather had a caregiver who came to his house when he was fighting cancer. I was in high school. It was the first time I had heard the word, so the associated image stuck with me.”

“When you think of the word ‘caregiver,’ what’s the first image that pops into your mind?” – Approximation of photos uploaded by men participating in a focus group of men in the general population.
Vance, 35, from Ohio, also thought immediately of “someone who cares for the sick or disabled,” as did Thomas, 47, from Minnesota: “I think of someone caring for an elderly person. Perhaps pushing them in a wheelchair or handing them their medicine.” Echoed Phillip, a 19-year-old student from Indiana, “I think nurses are the ultimate caregivers because it is their paid profession and they have the utmost experience.”
Seth, a 40-year-old man in the general population group who lives in rural Washington state, associated the word “caregiver” with “a low-pay nursing type worker, CNA. A nurse is a nurse. But a caregiver is a low skill, low-wage type of job.”
Geff, 51, who lives in the suburbs of Chicago, also posted a photo of a woman, but his was an image of a mother and child. “When my kids are sick, I help of course, but ultimately, they just want their mom. Mom makes it better. Mom knows. When I was little, I felt pretty much the same.”
Because of this narrow, feminine, and medicalized definition of care, many men in this general population group did not think of themselves as caregivers. But when asked about specific caring tasks, seven clearly were providing care to others. “I guess I am,” said Geff, who is the father of three. “I earn most of the money in the household, so I guess that qualifies.” Five of these men said they were not carers, though one said he was active in the “child-rearing” of his son. Thomas said he was not a carer “in the conventional sense of the word.” Rather, he spent a lot of time helping his wife and daughter, both emotionally and by “doing physical tasks that seem overwhelming to them.”
Because of this narrow, feminine and medicalized definition of care, many men in this general population group did not think of themselves as caregivers.

“When you think of the word ‘caregiver,’ what’s the first image that pops into your mind?” – Approximation of photos uploaded by men participating in a focus group of men who have cared for another adult.
Conversely, in the focus group of 14 men who had cared for an adult, the images men provided were wholly different. The men described caring for children, loved ones, spouses, aging parents, relatives, disabled friends, and neighbors in need, a clear indication that they saw caring as part of a relationship, whereas the men in the general population group saw caring as low-value work to be outsourced. The men who had cared for an adult further described the often intensive work they do—both hands-on care tasks like bathing, feeding, and medical treatments that are more commonly associated with women, as well as spending time with the person and managing financial, estate, household, and maintenance tasks. And all mentioned the joys as well as the pain and suffering that providing care to another involves.
Thirteen men in the group said that, in general, they spent more time caring for others than being cared for. One said he spent the same amount of time caring for others as he was cared for.
These men posted a variety of images showing a deeper, nuanced, and more personal relationship with care: people hugging, hands joining, family photos. Many posted photos of themselves with the wives, parents, or family members they provide care for. “Caregiving is all about family,” wrote Cody, who helps his aging parents with medical appointments, housekeeping, and maintenance.
Caregiving is all about family.
Matthew, 42, from Rockaway Beach, N.Y., has been caring for his mother since his father died. He takes her to the doctor, schedules activities, does her shopping, and makes sure she takes her medications. He posted a photo of the two of them at a wedding. “She was basically my date. And we had a blast. I try to include her in everything,” he said. The word “caregiving,” to him, meant “a smiling face on my mom.”
Andrew, 47, from Pennsylvania, who also cares for his mother, posted a photo of an embrace. “I think of a hug because that seems to capture the essence of caregiving, being ready to embrace and support a person who is in need.” He added: “I reflect on the times I was growing up and knowing she was there to provide. Now it’s my turn.”
I reflect on the times I was growing up and knowing she was there to provide. Now it’s my turn.
Richard, 45, from Port Huron, Mich., cares for an elderly neighbor with dementia, making sure he’s eaten, cleaning up after accidents, and spending time with him playing cards and keeping him company. He posted a silhouette of people supporting one another. “You have to love it,” he said of providing care. “I think being temporarily disabled myself has given me a unique insight. I am best suited as a caregiver just getting a smile (or not) when I leave.”
Oliver and Larry both care for their wives. Oliver, 42, a hotel manager who helps his wife with medical appointments, changes her dressings and manages her medications, posted a photo of two hands clasped. “Because my wife needs me to help her … I am offering a helping hand,” he said. “It’s a job that I love doing so much.”
Larry, 77, of Fairfax, Va., whose wife is beginning to suffer balance issues and hearing and memory loss, is doing more cooking and housekeeping in addition to caring for her and doing all the driving. He posted a photo of him and his wife. “It represents how true love is involved in the caregiving process.”
Andres, 37, lives in Ohio and does freelance work as a home care aide and cares for his son, elderly friends, and relatives. He posted a photo of two dishes of ice cream, because, he explained, it symbolized moments of providing care that were not only “very enjoyable,” but memories that changed him. The image is “savory and bittersweet because eventually, it had to end,” he wrote. “All care giver cases I have ever had the privilege of doing came to an end at some point, but each left an impression on both the other person I cared for and myself.”
Seeing is Believing for Men Learning to Provide Care
When we asked the men in the group of men who had cared for an adult what helped prepare them for their role giving care, exposure to role models was a key factor. These men drew from their own life experiences and cited the examples of their own parents caring, their own experiences of caring or volunteering for or with others, or seeing or interacting with paid or unpaid carers in action with family or loved ones as giving them the inspiration or guidance for shaping their views and behaviors around providing care.
“The way my parents took care of my grandparents. [That] instilled values in me to do the same,” said Matthew, who cares for his aging mother. Richard, who cares for an elderly neighbor, said he had been close to death twice himself, and the experience of being disabled and intensively cared for by others inspired his own empathetic style of care. “Having people take care of me in my time of need makes me understand in some small way what the gentleman is feeling.”
“When my mom was in the hospital for about 6 weeks, I tried to observe all that was going on and how the nurses took care of my mom. I asked questions to help prepare me for when she would be discharged to go home,” said Andrew.
Mark, 45, a FedEx contract driver from Atlanta who cares for his mother, began caring for family members at an early age, doing chores for his grandparents, then more intensively caring as they grew ill: “While I was in high school, both my grandparents were really sick and unable to stay in the house alone. So as an alternative to sending them to a senior care facility, they had a nurse who stayed with them during the day, while my two cousins and I took turns spending the night with my grandparents.”
In our focus group of fathers, Scott, 39, a single father from North Carolina, said that his experience working in the childcare industry helped him learn how to be a better father, “and also helped me be more patient and show more affection.” And Christopher, 42, a father of two boys and a network design engineer for a utility company in New York City, expressed a view more common among the men who had the experience of providing care for another when he said that experience itself is the best teacher. “I firmly think that there is some sort of hormonal bond between mother and child. ‘Maternal instinct,’” he said. “But just about anything can be learned. Remember the time you discovered the just-perfect speed to rock your child or the temperature that they like their milk?”
II. Men Who Care
Who They Are
Although women are still expected to be primary carers, the United States, in reality, is a nation of carers composed of people of all genders, including men. In our nationally representative survey, a large majority—nearly three-fourths of all respondents—identified as someone who provides care to a loved one.1
As a reminder, in analyzing our survey data, we found significant overlap in the number of people who have both ever cared for adults and parents who have ever provided care for a child with special needs, as well as in their attitudes and experiences. For these reasons, we grouped them together as High-Intensity Caregivers and /or Parents, HICP.
And though more women than men said they have ever cared for adults or children with special needs (56 percent), more than four in 10 men (45 percent) said they, too, have been responsible for this often labor intensive yet invisible and underappreciated care work. Although this gender difference is statistically significant, the finding that so many men are engaged in such high-intensity caregiving challenges the long-standing conventional wisdom that most men don’t provide care, don’t want to, or don’t know how to.
An additional 23 percent of our sample identified as parents who have never cared for a child with special needs, called Other Parents in this report, to distinguish them from the parents of children with special needs in the HICP group. This Other Parents group was evenly split between women and men (51 to 49 percent, respectively). And 26 percent of our sample were neither parents nor had they ever cared for an adult. This Non-Caregiver group was more male than female (59 to 41 percent, respectively).
Figure 2
The finding that 45 percent of men have ever cared for an adult as the U.S. population ages tracks with research by AARP and the National Alliance for Caregivers. They found two in five men, or 39 percent, had cared for an adult in the past 12 months, compared to 61 percent of women.
Just under 60 percent of those in our High-Intensity Caregiver and/or Parent, HICP, group who have ever cared for an adult or a child with special needs were employed, the same as the percentage of Non-Caregivers. Those in the Other Parent group—that is, parents who have never cared for a child with special needs—were more likely to be employed (71 percent). But there was no difference between the three groups in the share who worked part-time, full-time, or more than full-time. Almost a quarter of all three groups (including 23 percent of those in the High-Intensity Caregiver and/or Parent group) reported working more than 40 hours per week.
When asked “Have you ever provided ongoing or periodic living assistance on a regular basis to an adult family member or close friend,” men were more likely than women to say “no”—62 percent to 54 percent. Yet in keeping with the finding that America is a nation of carers, whether people recognize it or not, our survey found that even men in the Non-Caregiver group have in fact performed active caring tasks, as the following section will describe.
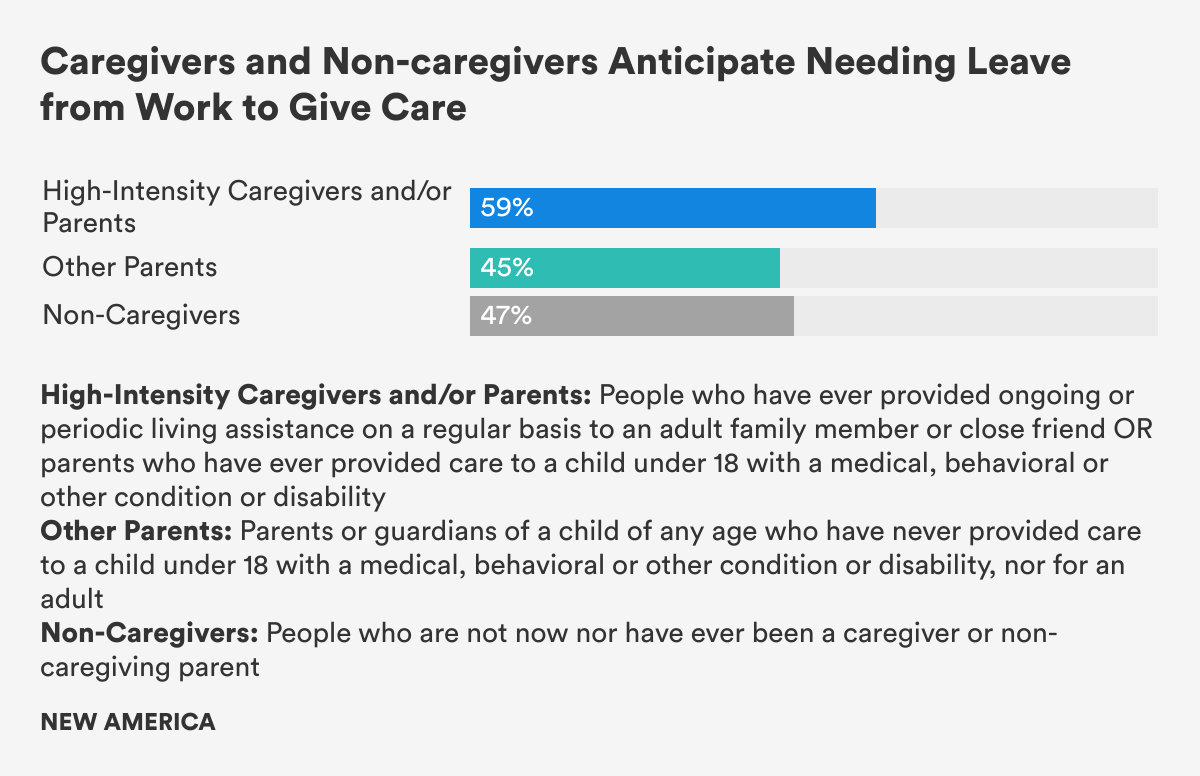
Moreover, large shares of people in all of our groups—High-Intensity Caregivers and/or Parents, HICP, Other Parents, and even Non-Caregivers—said that they anticipate needing time off work to give care in the near future. That includes not only 59 percent of HICP and 45 percent of Other Parents, but nearly half (47 percent) of those who do not have care responsibilities, suggesting that they anticipate that they will need to care for others in the future.
What Men Who Give Care Do: Pretty Much What Women Who Give Care Do
When it comes to what men who care actually do, research over the years has shown that men tend to do more hands-off tasks managing care, like home maintenance, car repair, and keeping track of finances. Fathers are more likely to play with children and be engaged in activities tied to learning and academics that are typically not bound by time deadlines. Mothers, on the other hand, are more likely to be responsible for much more of the task-heavy, time-bound day to day caring tasks of feeding, bathing, dressing, or administering care. So it may not be surprising that research has found that fathers tend to be less stressed and happier than mothers. Our research sheds new light on the tasks and activities that men who give care actually do, how they feel about it, and how it impacts their stress and health.
A previous Better Life Lab report on fathers found that large shares of fathers reported being actively engaged in both hands-on and hands-off parenting tasks. (That report was based on the same survey data but combined the data on all parents, regardless of whether they had cared for a child under 18 with a medical, behavioral, or other condition or disability.) Yet that report found that, on every measure of parenting tasks, mothers reported doing more than fathers by statistically significant margins on all tasks, save one—playing with children.
Our survey asked whether respondents had ever done any of the 15 “types of ongoing or periodic living assistance for an adult family member or friend who has/had a serious illness, or a disability, or needs extra help.” This list included two types of activities: “hands-off” tasks that keep the household running, keep the care recipient fed, and ensure the recipient gets medical care and medicine, and “hands-on” tasks that involve more intimate and medical care of the care recipient’s body. Hands-off tasks were much more common than hands-on tasks for both men and women. (Figures 3 and 4)
More than 90 percent of men and women in the High-Intensity Caregiver and/or Parent, HICP, group who have ever cared for an adult or child with special needs reported ever having done any of eight hands-off caring tasks, and the average number of these tasks men and women reported doing was the same (five). The only statistically significant differences between men and women in this group for hands-off caring tasks were for providing transportation outside the house and for household maintenance like mowing or fixing things, reported by 72 percent of HICP men and 58 percent of HICP women.
There was slightly more evidence of gendered caring when it came to the hands-on tasks: 72 percent of women who are High-Intensity Caregivers and/or Parents, HICP, performed hands-on tasks compared to 62 percent of HICP men. However, it’s important to note that nearly two-thirds of men who care for adults or parents of children with special needs are also performing intimate hands-on care tasks—a far higher share than predominant cultural stereotypes of men as absent or unwilling providers of care. Similarly, women who are High-Intensity Caregivers and/or Parents, HICP, reported performing 2.1 hands-on tasks on average, whereas men with these same care responsibilities reported performing 1.7 hands-on tasks. While this difference is statistically significant, meaning that it is unlikely to be due to random chance, it still amounts to a difference of less than one task between the genders.
It is important to note that we asked whether someone had “ever” done these care tasks, and did not capture how much or how often someone performs them. Time diary research shows that women spend about twice as much time on housework and caring than men do. Still, when it comes to the types of care tasks, we found that men who care for adults or fathers of children with special needs are more similar to women with the same care responsibilities than cultural stereotypes may recognize.
… are more similar to women with the same care responsibilities than cultural stereotypes may recognize.
In terms of specific hands-on caring tasks, there were only two significant differences between men and women who care for adults or parents of children with special needs. Women who are High-Intensity Caregivers and/or Parents, HICP, were more likely to administer medicine than HICP men (50 percent of women vs. 40 percent of men), just as HICP women were more likely to bathe, dress, and help with toileting (50 percent of HICP women vs. 35 percent of HICP men.) For all other hands-on tasks, there were no other statistically significant differences between the genders.
Figure 3
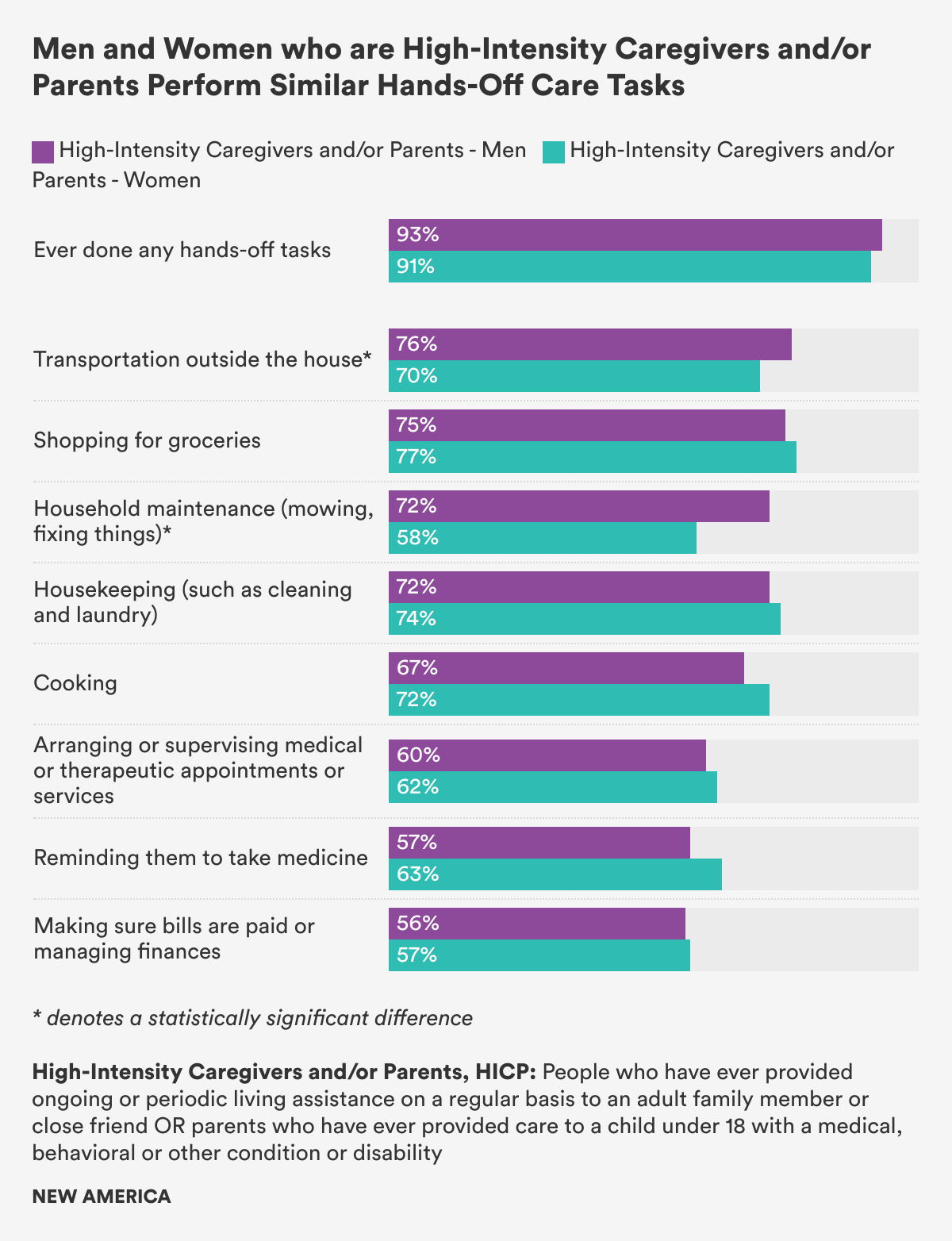
Figure 4
Non-Caregivers Also Give Care
More than half of the Other Parents who have never cared for a child with special needs (58 percent of fathers and 65 percent of mothers in this category) and nearly a quarter of the Non-Caregiver group had nevertheless performed hands-on caring tasks for an adult. Just as for those in the High-Intensity Caregiver and/or Parent group who have ever cared for adults or children with special needs, the most common hands-on tasks performed by those in the Other Parent and Non-Caregiver groups were administering medicine, changing bandages, and assisting an adult with bathing, toileting, and getting dressed.
Among Other Parents and Non-Caregivers, the only statistically significant gender difference in terms of caring tasks is that men in both groups were more likely than women in both groups to perform household maintenance. (Figure 5)
It is interesting to note that so many individuals who do not identify themselves as caregivers are actually doing so many hands-on and high-intensity caregiving tasks for adults. That may indicate that they’ve provided occasional help, or that they may have a limited view of care. Our focus groups, as discussed in section one, illustrated this point as well: A number of men in the general population group didn’t see themselves as caregivers, even though, upon reflection, they were performing many caring and/or parenting tasks.
Figure 5
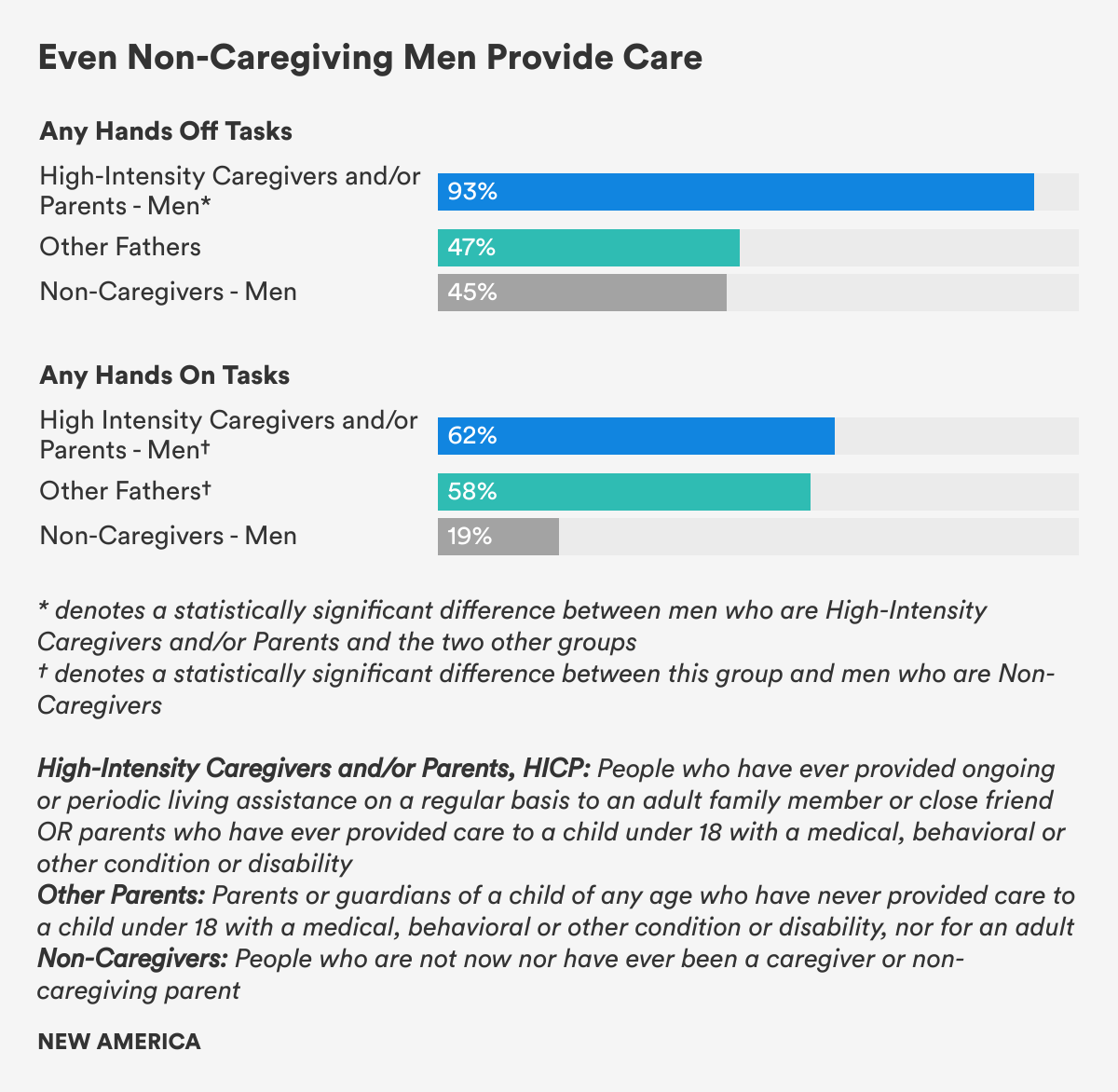
Though we found few gender differences, we did find that the family care responsibilities at home are often much more demanding for men who are High-Intensity Caregivers and/or Parents, HICP, than for the men in the other two groups. Men who care for adults or fathers of children with special needs performed up to six times more caring tasks than Other Fathers and men who are Non-Caregivers by a statistically significant margin on each of the 15 different caring tasks.
… performed up to six times more caring tasks than Other Fathers and men who are Non-Caregivers.
For instance, men who are High-Intensity Caregivers and/or Parents, HICP, perform far more hands-on and hands-off tasks: 93 percent of HICP men say they have ever done any hands-off tasks, averaging 5.3 tasks, compared to 47 percent of Other Fathers, who averaged 2 tasks. And 62 percent of HICP men say they have done the more intensive and intimate hands-on tasks, compared to 25 percent of Other Fathers. Understanding these differences in hands-on caring is critical, as previous research has found that men say they are untrained and find aiding with personal care most stressful of all caring tasks.
Men Need Paid Family Leave in Order to Care
More High-Intensity Caregivers and/or Parents, HICP, who have ever cared for an adult or a child with special needs said they had used paid family and medical leave from work to give care (41 percent) than Other Parents who have never cared for a child with special needs (27 percent). But in both of these groups (HICP as well as Other Parents), men and women were equally likely to have used paid time off to provide care. However, other research shows that the vast majority of workers do not have dedicated paid family and medical leave to care for a new child or an ill or disabled loved one.
While policymakers look for solutions, our data provides critical evidence of the need for comprehensive paid family and medical leave as they consider public paid leave policy options. Our data shows that the inclusion of paid leave for family care responsibilities is critical. The leading federal policy proposal, the Family and Medical Insurance Leave Act (FAMILY) Act, and several state paid family and medical leave programs include up to 12 weeks of paid leave for family care responsibilities—responding to this widespread need. However, the paid leave program Congress enacted for federal employees, and some alternative paid leave proposals pending in Congress, cover only new parents who need to provide care for a newborn or newly adopted child. As our data shows, there is a vast swath of people who are struggling to combine work and intensive, sometimes years-long care responsibilities—and this important constituency would be excluded from paid leave proposals that cover only new parents. The universe of people who need paid family leave may be even bigger than surveys show: Even 16 percent of people who have never given care, the Non-Caregiver group in our study, said they had taken a paid leave from work to give care.
The universe of people who need paid family leave may be even bigger than surveys show.
Research has found that when men take paid leave, their spouses and partners are more likely to return to work, enjoy better health, and advance in their careers. Thegender pay gap also narrows. One study of families in Sweden even found that for every month of leave a father takes, his partner’s earnings increase by 6.7 percent.
Indeed, many men who take paid parental or paternity leave tend to become more involved in care work, willing to work flexibly and share care with their partners, which, over time, not only increases gender equity at work and home, but as research shows, has led to better relationships, less family stress, healthier, happier children, and even longer lives for men.
In our previous Better Life Lab report exploring men and paid family leave, one of the most surprising findings is that men anticipate needing to take time off work to care for loved ones just as much as women do. Three in 10 men and women surveyed expected needing to take time off work in the future to care for a new baby. And half of the respondents—men and women alike—anticipated needing time off to take care of a sick, disabled, or elderly family member.
One of the most surprising findings is that not only do similar shares of men and women with care responsibilities anticipate needing to take time off work to give care in the future but so do similar shares of men and women who have no care responsibilities. (Figure 6) In all three groups—High-Intensity Caregivers and/or Parents, HICP, Other Parents and Non-Caregivers—there is no difference by gender in the share of those who anticipate needing to take leave from work to give care, whether following the birth or adoption of a child or to care for an adult or family member with a serious illness or disability.
In our focus groups of men with care responsibilities and subsequent research, we heard stories of men longing for their own “maternity leave,” wishing they had had more supportive workplaces so they could have more time with family. Several men related the sometimes outrageous lengths they had to go to—saving up sick days for years, draining vacation time, even quitting jobs—so they could take some time off work to care for the people they love.
Many said taking leave was critical not only to be the kinds of fathers and sons they wanted to be but for their wives and partners to live the kind of lives they had hoped for. The main reason people said men take leave from work to provide care—84 percent—is because it’s the right thing to do. Some men in the focus groups say they’re filled with “guilt and resentment” that their inability to take adequate parental leave set the stage for their wives and partners to become the primary carers, forced to dial back at work in order to carry the heavier load at home.
Many said taking leave was critical not only to be the kinds of fathers and sons they wanted to be, but for their wives and partners to live the kind of lives they had hoped for.
Joe Ferrante, one of our focus group members who agreed to a longer follow-up interview and to be identified by name, is a mortgage banker based in New York. He believed he was one of the small share of men in the United States actually covered by a firm’s voluntary paid paternity leave policy—13 percent—but he did not realize the limits of that policy. First, the company didn’t make it easy for him to find out about, much less actually use it. And then, just before his parental leave was to start, he learned that his company would only cover his minimum-wage base salary if he took paternity leave, rather than compensate him for his paternity leave at his usual higher rate, which took into account the commission he relies on to pay his bills. He was so angry that he quit. “My manager told me, basically, ‘Look, just take sick days and vacation days, and that’ll cover the time,’” he said. “I thought that was ridiculous. That took away from my vacation. I should’ve gotten my regular paternity leave.” Joe’s story illustrates that even the disproportionately well-paid professional men who are more likely than others to have paid parental leave may not be able to use it.
Even Richard Petts, a sociology professor at Ball State University who studies men and care, said in an interview that he had trouble taking time off under the university’s family leave policy. “I was told if I wanted to take a day or two off, that was fine. If I wanted to take more time, I would need a note from my wife’s doctor saying that she was incapable of taking care of our child.” That was in 2012.
If I wanted to take more time, I would need a note from my wife’s doctor saying that she was incapable of taking care of our child.
Dave Sucharski, a man in our focus group of fathers who agreed to a follow-up interview and to be identified by name, felt anguish that he did not have access to paid paternity leave when his wife gave birth after a difficult labor. Though their daughter was in the neonatal intensive care unit, he was back at work after he’d used up a week and a half of his vacation time. His wife was forced to take unpaid leave, because, he said, someone had to care for the baby. “I just don’t think it’s accepted by society, by the business world, that this is something a husband, a man, should do,” Sucharski said. “There’s pressure that that’s not my job. My job is to be the breadwinner. Not to be home with ice packs and baby bottles. It’s really sad and really frustrating to me. I just wish I could have spent more time at home.”
And consider the story of Jay Lane, a man who shared his experience of care in the COVID-19 pandemic in an interview. Lane left his job as an assistant gas station manager in Maryland after his managers rejected his request to take unpaid leave through the Family and Medical Leave Act, as he was entitled to under federal law. Though Lane felt strongly about being present for his then-fianceé after the birth of their daughter and had been saving up for months to be able to afford unpaid leave, he still expected to be the primary breadwinner and his partner to take on all the care duties. His “help,” he expected, would be temporary at most.
But when the pandemic hit, he was furloughed from a new job and he began sharing care equally with his partner. The experience itself changed him. He's not only shared tasks like laundry, dishes, cooking, and feeding and changing the baby (“I never realized how many diapers a baby can go through. I never realized how much work it is to take care of a baby.”), he’s also watched her learn to crawl, take her first steps, and begin to talk. Now, he’s noticed that his daughter will seek him out to soothe her, play with her or help her sleep, whereas when he was working full-time before the pandemic, she gravitated toward her mother. Lane is now planning a much different return to work, one that will enable him flexibility and time to continue to be engaged in care work. “I want to make sure I keep building those bonds with her,” he said, “so that she can count on me as well.”
Figure 6
Citations
- While the survey and focus group data report on men and women as a binary, the Better Life Lab recognizes gender identity as a spectrum and respects nonbinary identities and people of all genders.
III. Men and Work-Family Conflict: The Heavy Toll on Men who are High-Intensity Caregivers and/or Parents
Work, Not Care, is the Main Source of Work-Family Conflict
Men who give care—High-Intensity Caregivers and/or Parents, HICP, as well as Other Fathers—report up to four times more work-family conflict than men who are Non-Caregivers, another key indicator from the survey data about how the experience of providing care can shape men’s lives. (Figure 7) Just 10 percent of Non-Caregiving men, for instance, reported feeling that they had to put off work because of the demands on their time at home, compared to 41 percent of HICP men and one third (33 percent) of Other Fathers.
A key finding, however, is that among men who care, men who are High-Intensity Caregivers and/or Parents who have ever cared for adults or children with special needs experience more work-life conflict and stress and lower levels of pride and satisfaction with their caring roles than do Other Fathers who have never cared for children with special needs. Men who are High-Intensity Caregivers and/or Parents, HICP, are also as likely as HICP women to miss work or reduce work hours due to care demands. In this section, we will explore work-life conflict, satisfaction with care, and burnout by gender and care experience, and how men’s stronger ties to work and breadwinner identity make it difficult, or seem impossible, for many of them to find time to both work and care.
When it comes to work-family conflict, researchers have identified two primary modes: work-to-family conflict, when the demands of work spill over and take away time for life, family, and care; and family-to-work conflict, when family responsibilities spill over and interrupt time and attention from work.
In a sign of the large influence the American overwork culture has in our lives, all three groups—High-Intensity Caregivers and/or Parents, HICP, Other Parents and Non-Caregivers—experienced far more work-to-family conflict than family-to-work conflict, meaning work disrupts home life far more than care work gets in the way of paid work. These findings reinforce research showing that both work and family are “greedy institutions” that demand time, attention, and energy, but that, in the United States, where there are no public policies guaranteeing paid annual leave, paid sick or paid leaves for care, and where work hours are among the longest of any advanced economy, work is the greedier institution.
Figure 7
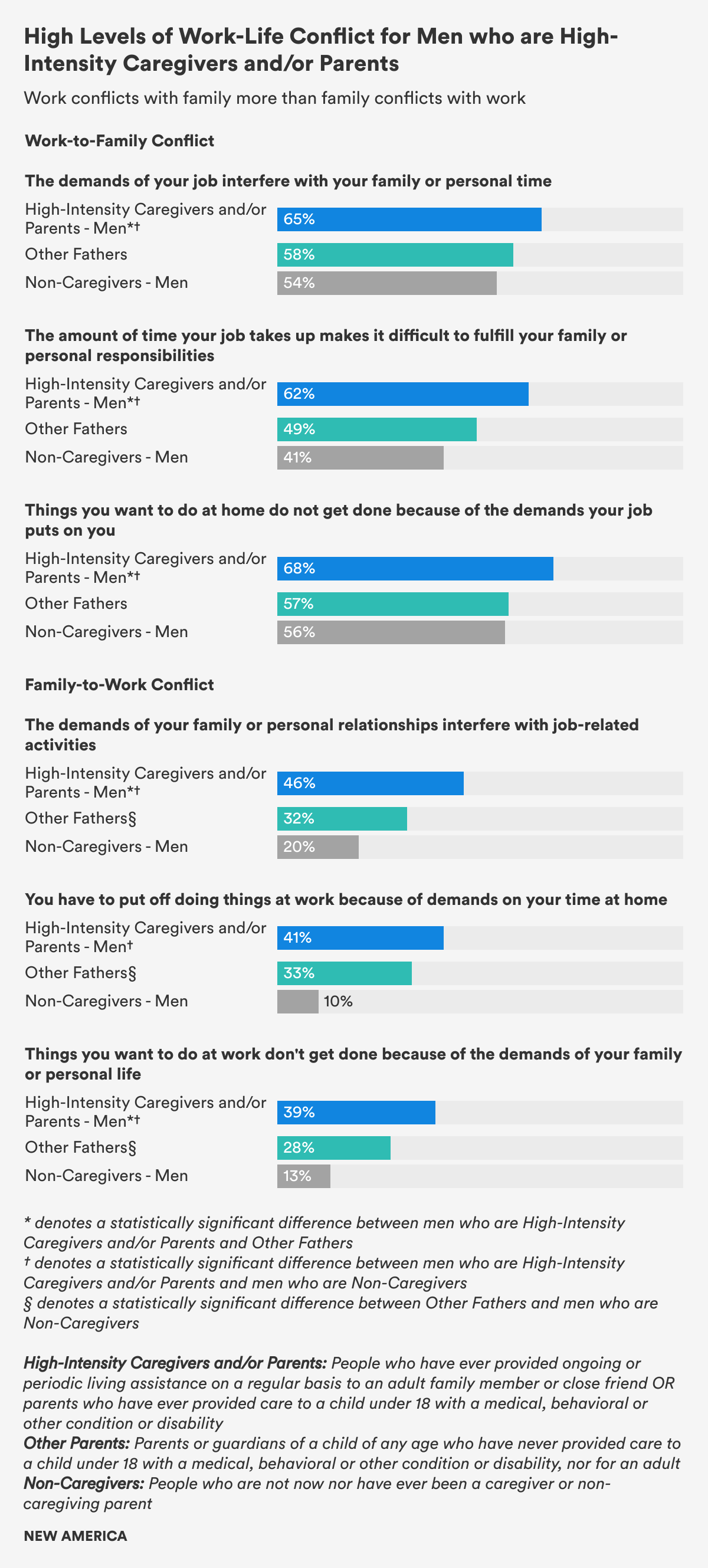
For instance, about twice as many men who are High-Intensity Caregivers and/or Parents, HICP, (65 percent) and Other Fathers (58 percent) said the demands of their job interfere with their family or personal time than reported that their family responsibilities interrupt their work, which was noted by 39 percent of HICP men and 28 percent of Other Fathers. Given that men in the HICP group perform so many more care tasks (as described in section two), it is noteworthy that HICP men are still more likely to say that work interferes with family responsibilities, rather than family responsibilities interfere with work.
Perhaps most importantly, we found that large shares of employed men who are High-Intensity Caregivers and/or Parents, HICP, reported missing work, reducing work hours or leaving the workforce entirely because of care duties. (Figure 8) While 71 percent of employed HICP women said they had missed work to provide care, so had 64 percent of HICP men—and this difference between genders was not statistically significant. More than 40 percent of employed High-Intensity Caregivers and/or Parents of both genders had reduced their work hours to provide care, and more than 50 percent of employed High-Intensity Caregivers and/or Parents of both genders had left the workforce or retired early to provide care.
Figure 8
Men who are High-Intensity Caregivers and/or Parents Experience More Work-Life Conflict
Providing care to loved ones and others is a complicated experience. Care work can be physically, emotionally, and mentally draining, depleting, exhausting, and lead to burn out. It can, at the same time, also be a source of great joy, satisfaction, pride, connection, and meaning. In our survey, 85 percent of High-Intensity Caregivers and/or Parents, HICP, who have cared for an adult or a child with special needs and Other Parents who have never cared for a child with special needs found their care work satisfying. Nearly 90 percent of High-Intensity Caregivers and/or Parents, HICP, and Other Parents said they felt respected inside and outside their families for their care work, though fewer of the youngest carers and parents in both groups ages 18 to 29—67 percent—felt proud to talk about their caring roles compared to 81 percent of those ages 30 to 44.
However, in our survey data, we found significant differences in the experiences of High-Intensity Caregivers and Parents, HICP, and those of Other Parents when it comes to both the stresses and joys of care work. These differences between these caregiver groups transcended gender lines, although there were a couple of notable gender differences.
On five of the six work-family conflict measures, High-Intensity Caregivers and/or Parents, HICP, experienced more work-life conflict than Other Parents. For instance, roughly two-thirds of both HICP men and women reported that the demands of their jobs made it difficult to fulfill family or personal responsibilities, compared to 49 percent of Other Parents. Among High-Intensity Caregivers and/or Parents, HICP, men and women were equally likely to experience work-family conflict: There were no statistically significant differences by gender.
In looking only at men, we found statistically significant differences between men who are High-Intensity Caregivers and/or Parents, HICP, compared to Other Fathers on every measure, save one: burnout. HICP men felt less respected for their care work than Other Fathers both inside and outside of their families. And compared to Other Fathers, HICP men reported higher levels of stress, lower levels of satisfaction, and fewer opportunities for growth in their care work—an indication, perhaps, that while parenting a child with no special needs can be exhausting, it is also ultimately a joyful and meaningful experience watching a child grow to independence. Caring for a child with a medical, behavioral, or other condition or disability, or for an older adult in declining health is perhaps no less meaningful, but can also be much more demanding, stressful, and time-intensive.
Figure 9
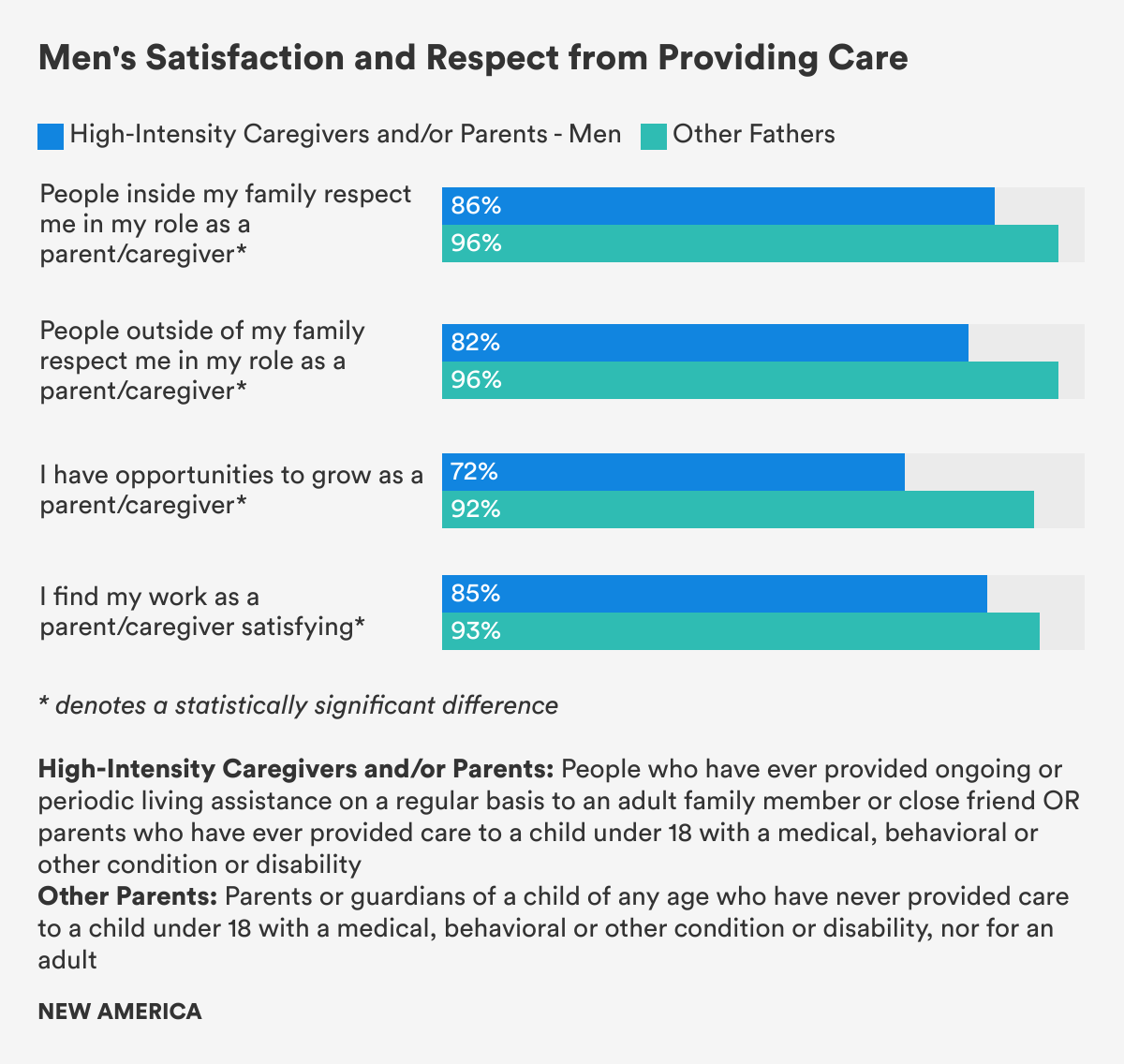
When it comes to gender differences, though the percentages are still quite high, fewer men who are High-Intensity Caregivers and/or Parents, HICP, felt respected by people outside their families than HICP women by a statistically significant margin (82 percent of HICP men to 88 percent of HICP women). And among the Other Parents, significantly more of these mothers (98 percent) felt they had opportunities to grow as a parent compared to these fathers (92 percent). In contrast, about 70 percent of HICP men and women felt they had opportunities to grow as caregivers.
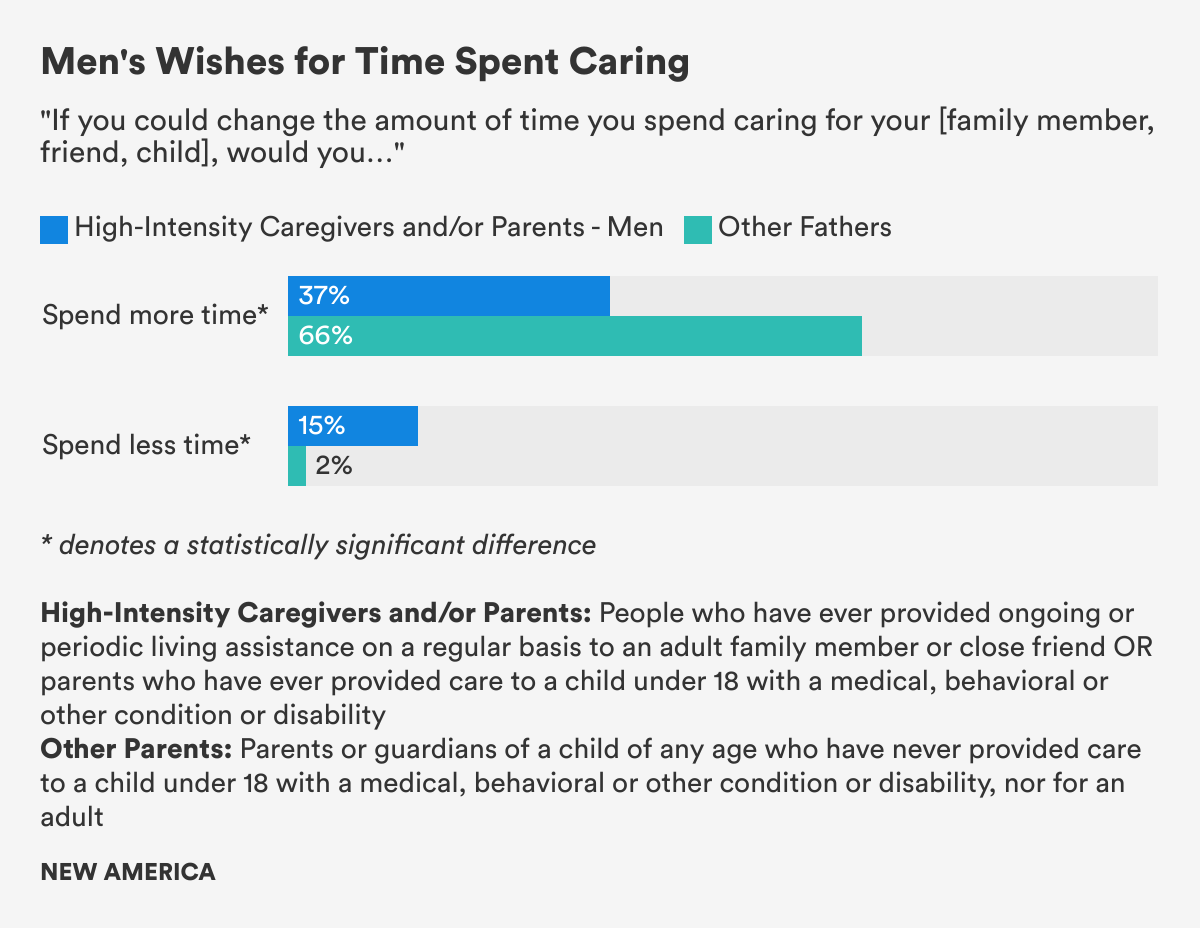
High-Intensity Caregivers and Parents, HICP, were also less likely than Other Parents to say they would like to spend more time caring—53 percent of Other Mothers and a substantially higher two-thirds of Other Fathers said they wished they could spend more time caring for their children. That contrasts with just 34 percent of HICP women and 37 percent of HICP men. Fifteen percent of men who are High-Intensity Caregivers and/or Parents, HICP, and 18 percent of HICP women said they wished they could spend less time caring, compared to a scant 2 to 3 percent of Other Parents.
Figure 10
Two-thirds of High-Intensity Caregivers and/or Parents, and Other Parents Feel Burned Out by Care Demands
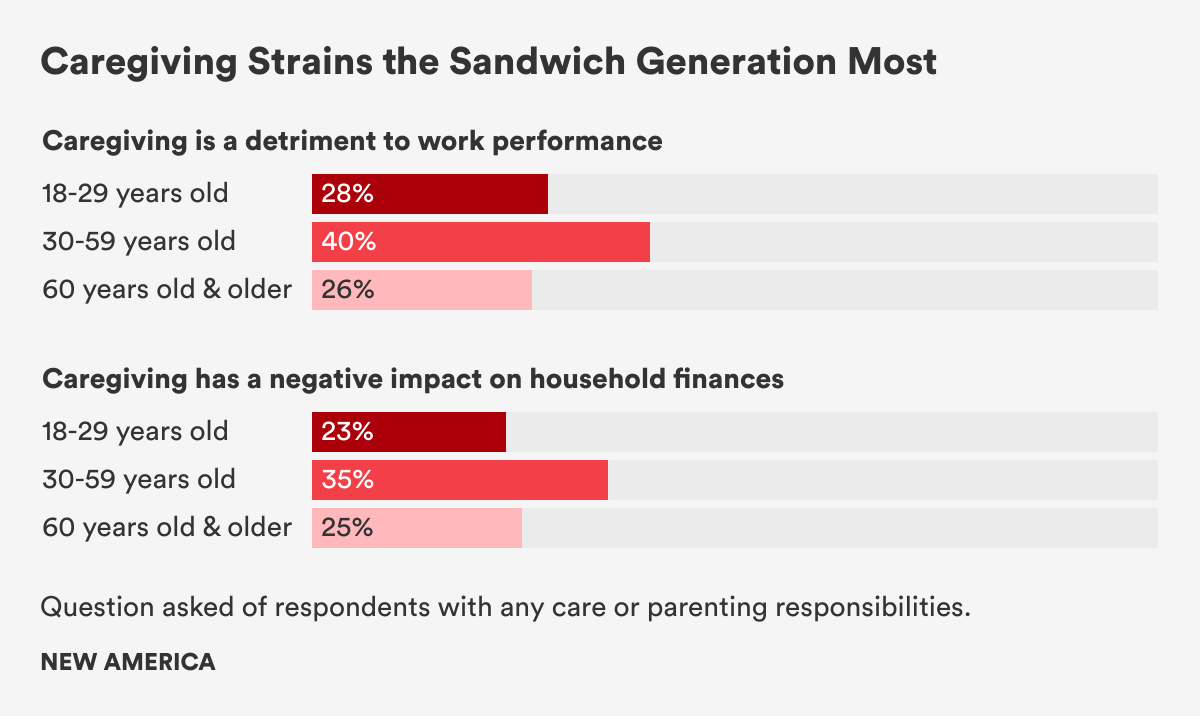
More than six in 10 High-Intensity Caregivers and/or Parents, HICP, reported feeling burned out from care responsibilities at least sometimes or said that it’s more stressful than other work. Nearly half reported that care work has negatively impacted their stress and mental health, while 32 percent reported a negative impact on physical health and 30 percent on family finances. Respondents between the ages of 30 and 50—the height of the “frenzied families” era of care responsibilities as parents and sandwich generation carers for aging parents or loved ones—said care work was more likely to have a detrimental effect on their paid work and family finances compared to those in younger and older age groups.
Families that care for aging adults and people with disabilities face difficult financial struggles. A 2016 survey by AARP, for instance, found that family carers spend about 20 percent of their income on care activities, amounting to about $7,000 per year in out-of-pocket expenses.
Figure 11
Among High-Intensity Caregivers and/or Parents, HICP, who have ever cared for an adult or child with special needs, 64 percent of women and 58 percent of men say they feel burned out by their care work. Similarly, among Other Parents who have never cared for a child with special needs, 65 percent of these mothers and 60 percent of fathers said they feel burned out by their care duties.
Although our survey found similarly high levels of burnout for High-Intensity Caregivers and/or Parents, HICP, and Other Parents, previous research has found that parents of children with special needs are at higher risk of burnout than parents of children with no special needs. Research has also likened the chronic stress that mothers of disabled adolescent children experience to the stress of combat. Fathers of children with special needs, likewise, have been shown to experience far higher stress levels than fathers of children with no special needs. Fathers whose children have chronic illness or disability can have what’s been described as “hunter-provider anxiety”—a fear of failing to find or keep a regular job while at the same time balancing the often high financial costs and time demands of care responsibilities.
Research has also likened the chronic stress that mothers of disabled adolescent children experience to the stress of combat.
This research has also found that the three keys to mitigating stress and burnout, particularly for those who care for adults, include being supported by family and friends, having time to rest and recuperate, and feeling appreciated by those whom one is caring for.
In our data, we asked High-Intensity Caregivers and/or Parents, HICP, if they had support for their often heavy caring duties. HICP men and women reported having roughly similar levels of emotional support. About 45 percent of men and women said they had “lots of people” they can talk to about their care responsibilities—a surprising finding, given that previous research has found that men are less likely to have social networks or feel comfortable talking about concerns about their care responsibilities, which can lead to feelings of isolation. Sons caring for elderly parents have higher levels of emotional and financial strain, compared to fathers or spouses.
Figure 12
As far as physical support or sharing the load, about one-third of men and women who are High-Intensity Caregivers and/or Parents, HICP, said they do not have others they can count on to help them with their care duties.
One-third of men and women who are High-Intensity Caregivers and/or Parents, HICP, said they do not have others they can count on to help them with their care duties.
In terms of support, the only statistically significant difference we found between genders for High-Intensity Caregivers and/or Parents, HICP, was in their access to resources to enable them to take a break when they need it. Far more HICP men, 53 percent, said they had access to resources to give them a needed break than HICP women, 40 percent.
What to make of that? It could be that because of men’s higher earning power—fueled by the gender pay gap that rewards men and male-dominated professions more than women and female-dominated ones—and the traditional masculine identity tied to finances and breadwinning, they have the power to pass off care duties to women when they need a break, whereas women are less likely to be able to do so. Or that men who are High-Intensity Caregivers and/or Parents, HICP, are more likely than HICP women to have the financial resources to hire others or outsource care when they need respite, as well as the expectation that they deserve to rest. Women, as previous research has found time and again, not only have fewer resources, but they feel more responsible for care work, tied to their traditional role as carers, feel less entitled to take time off for rest or to take care of themselves, and are more likely to feel guilty admitting that they even need it.
Men who are High-Intensity Caregivers and/or Parents Need Support at Work to Manage Work-Life Conflict
In our focus groups, men’s stronger ties to paid work over care work, and the expectation that they should prioritize financially providing for others came through clearly. In the general population focus group discussions, men tended to believe it was more difficult to combine full-time work and caring than women did, with eight out of the 13 men saying it would be impossible or difficult. Just two out of 13 women in the general population group similarly said it would be difficult to combine full-time work with care responsibilities, but quickly went on to imagine how flexible schedules and supportive bosses and coworkers could help make it work.
“There is no way I could continue with my current job and being a caregiver. My job is far too demanding on its own. If I had to provide this care, I would likely need to take a leave of absence or resign. And that certainly introduces financial and health insurance issues for me and my family. A supportive employer with a good leave policy would be required,” said Geff.
In the focus group discussion among men who care for an adult, many men in this group as well couldn’t see a way to combine full-time work and care responsibilities. “I don’t think I could do it all the time … especially with a full-time job. I think I would need time and training to make it possible, or to be two people,” said James, who cares for his mother.
But unlike the men in the general population group, the men who had cared for an adult began to imagine what they would need to combine work and care, including flexible schedules, and supportive managers and work environments. Still, the men in this group had a clearer understanding of the toll combining work and care takes than those in the general population group of men. “There is not enough time in the day for those two jobs to make it a reality,” said Oliver, who cares for his wife. “If I was working full-time caring for an adult and at the same time working my regular full-time job, I would be burned out quickly.”
IV. An Overwhelming Majority of Men Value Care and Believe it Should be Equally Shared. But Belief Isn’t Associated with Practice.
We asked a series of questions to try to unearth how men valued care, and whether having the experience of giving care would be associated with men valuing it more. Or, conversely, if men valued care, whether that would be associated with them actually giving it. We didn’t find that. Instead, we found that men fairly universally said they value care—men who are High-Intensity Caregivers and/or Parents, HICP, Other Fathers, and Non-Caregiving men alike. And an overwhelming majority of men—more than 80 percent—regardless of their caregiving or parenting experience and across racial and ethnic identity believe that men and women should share care responsibilities equally at home.
And yet, we found that that belief doesn’t translate into actually giving care.
Men Overwhelmingly Value Care
Overwhelming majorities of men—men who are High-Intensity Caregivers and/or Parents, HICP, who have ever cared for an adult or fathers who have ever cared for a child with special needs, Other Fathers who have never cared for a child with special needs and men who are Non-Caregivers—agreed that the care work people do at home is valuable to society, ranging from 84 percent of Non-Caregiving men to 91 percent of Other Fathers. Large majorities of men also said that the care work people do inside the home is as valuable as the paid work others do outside the home, ranging from 79 percent of Non-Caregiving men to 87 percent of men who are High-Intensity Caregivers and/or Parents, HICP. That so many men value care work as much as paid work is a surprising finding, given the powerful cultural norms that tie women to unpaid care work and men to paid breadwinning work in a society that has long undervalued care as a “labor of love” and equated success and power with the ability to earn income. But it could also be a reflection of men valuing care in the abstract or the care that others give without necessarily connecting the question to their own role, identity, or the expectation that they give it.
Large majorities of men also said that the care work people do inside the home is as valuable as the paid work others do outside the home.
A majority of people in all three groups espoused egalitarian views: 88 percent of women who are Non-Caregivers said care work is as valuable as paid work, compared to 79 percent of men who are Non-Caregivers. Among High-Intensity Caregivers and/or Parents, HICP, and Other Parents, there was not a significant difference between genders, with more than 80 percent of men and women sharing this view.
There was also more similarity than difference along racial and ethnic lines, with more than 80 percent of Black, Latino, and white men who are High-Intensity Caregivers and/or Parents, HICP, saying that the care work people do at home is valuable to society.
Figure 13
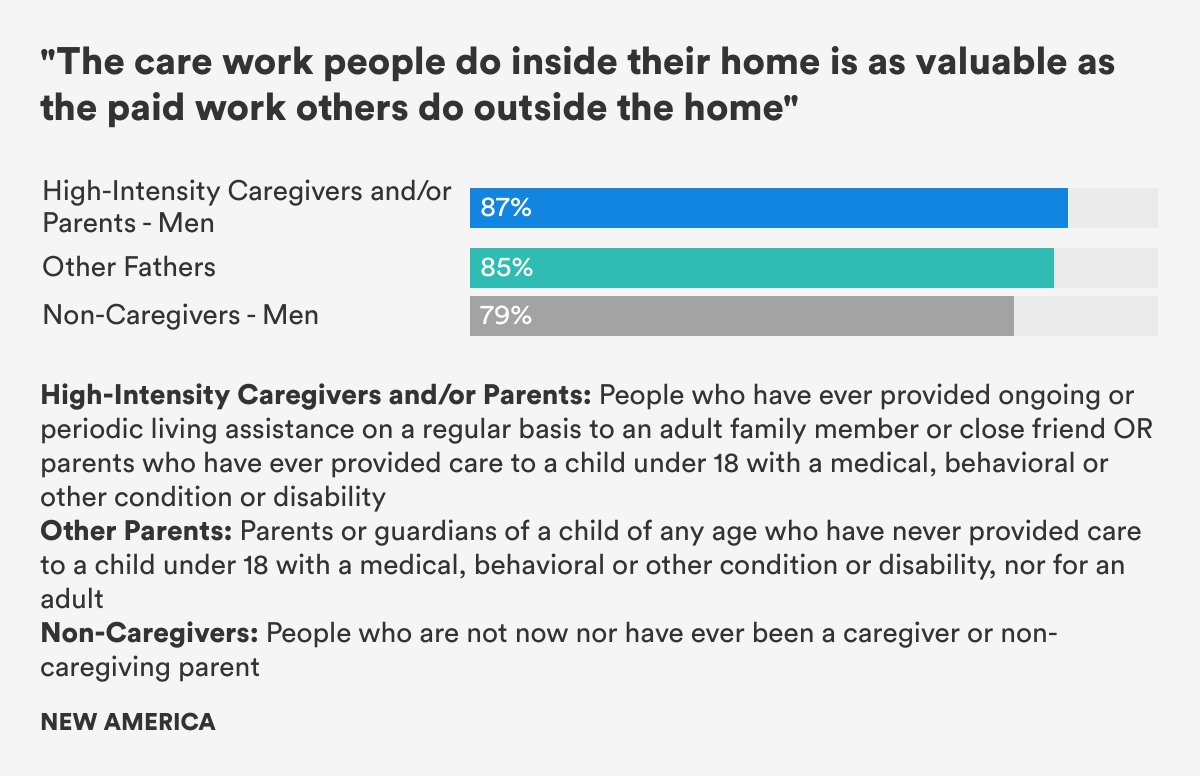
Additionally, those who were older or had more income were also more likely to agree that care work is as valuable as paid work and that care at home is valuable to society. Men and women over age 44, regardless of care experience, valued care at higher rates than those younger than 44, a sign perhaps that the idea of care becomes more valuable as one becomes more likely to give it, or to need it. And, again regardless of care experience, those earning more than $100,000 were more likely to say care work is valuable to society and as valuable as paid work than were those earning less than $30,000, an indicator, perhaps, that financial stability, and freedom from constantly worrying about putting food on the table or paying the rent, is a key precursor to enabling more men and women to see the value of care. Or it could be a sad indicator that, in the United States, the ability to provide care is a privilege.
We asked our focus group of men who care for adults whether they felt society respects and values the work they do caring for another adult. Four said yes. Four said no. “I don’t think society appreciates the caregiver until it’s time to be cared for,” said Justin, 39, from Atlanta, who cares for his father who has mobility issues. And six said they either didn’t care what society thought or that society doesn’t understand them.
I don’t think society appreciates the caregiver until it’s time to be cared for.
Matthew, who cares for his widowed mother told us, “Nothing makes me prouder [than] knowing she’s proud of me.”
Men Have Strong Egalitarian Beliefs. Yet Traditional Gender Norms Hold Sway
As we noted in our earlier Men and Care report on fathers, there are wide discrepancies between what men say they believe and what they do: 91 percent of men and women in our survey agreed that care work should be divided equally between men and women. Yet, just 46 percent said that is what actually happens when a family member needs care. And, as other surveys have found, men were nearly twice as likely as women to see the division of care labor as equitable—60 percent of men compared to 32 percent of women.
Still, the egalitarian ideal is strong: The vast majority of survey respondents, regardless of their care experience, say that men and women should divide care responsibilities equally at home: close to 90 percent of men in all three groups. Women in these groups agreed at about the same rates.
This egalitarian ideal is held across all racial and ethnic groups, income groups, ages, geographic areas—rural, urban, and suburban—and political party affiliation, with more than 80 percent of respondents in each category saying that men and women should divide care work equally.
Yet, in our focus group discussions, men and women alike, regardless of their experience of providing care, expressed the traditionally gendered view that women are naturally suited to care. While both men and women said that men are as capable of providing care, many believed that women possess inherent traits that men lack. Eight of the 13 men in the general population focus group thought of women as having a “maternal instinct” or that women are more “nurturing” or “compassionate” than men. And nine of the 14 men who care for adults also held this view, as did eight of the 14 women in the general population focus group of women.
Still, when we asked men who care for adults if their care experience would be different if they were women, nine said no. Nicholas, a 36-year-old man from Virginia who helps care for his father, said that taking care of others shows that a “man or woman can be very similar when it comes to giving support of their loved ones.” Mark, the FedEx driver from Atlanta who cares for several adults, including his parents, grandfather, and a nephew with mobility issues, even as he nodded to believing that women may possess innate qualities for care, said that that doesn’t matter. “Women have a maternal instinct that could factor in them being better caregivers, but I think it’s up to each individual person and the makeup of their character and willingness to sacrifice for someone else.”
I think it’s up to each individual person and the makeup of their character and willingness to sacrifice for someone else.
Of the five men who care for adults who thought their experience would be different if they were women, three specifically mentioned that it is society’s expectations, not an inherent skill, that makes the experience of providing care different by gender. “I think people are not as used to men as caregivers. People prejudge without realizing. They think women are better,” said Cody, who works in logistics and cares for his aging parents. Added Malachi, a 32-year-old from Chicago who cares for his father with advanced Alzheimers, “I believe if I was a woman, it may be accepted more in society, as women are seen as the caregivers for families.”
And in our focus group of fathers, all 14 believed that, in addition to a “maternal” instinct, there is also a “paternal” instinct. Again, some fathers pointed to societal expectations for shaping unconscious bias and the view that women are more suited to care. “I think that the unconscious prejudices in society have made the historical mothers’ role more important to be filled by a female,” said Kyle, 36, a manager at a logistics company in Massachusetts. “I think there has been progress made but there is a long way to go for it to be seen as equal.”
In a potentially important sign that the experience of providing care can shape men’s beliefs, biases, and attitudes, more men who had cared for an adult than the men in the general population focus group believed that women were not more likely than men to possess any skills important to being a good carer. Only two men in the general population group held that view, while the majority believed women are more naturally empathetic and compassionate, so better at caring.
Yet in the group of men who care for adults, opinions were more divided, with six men disagreeing, sometimes vehemently, that women have skills important to caregiving that men don’t have. “No!” said Larry, who cares for his aging wife. “None that I could think of … whatsoever,” said Oliver, who also cares for his wife. Others believed that men may have instincts that workplaces and traditionally gendered cultural expectations don’t allow them to fully develop.
Andres, who cares for two elderly men in his community, in a view that others applauded, said that men and women both have instincts to care for others. “But a man’s instinct in that realm doesn’t kick in until there is something worth caring for present in their lives. Most women I have met do not need to tap into that instinct. Men seem to have to learn that skill vs. already having it.”
Twice as Many Men as Women Say Society Doesn’t Trust Them to Give Care
Men who are High-Intensity Caregivers and/or Parents, HICP, and Other Fathers were twice as likely as HICP women and Other Mothers to report pushback to their caring because of their gender. One in five men (21 percent) who were either High-Intensity Caregivers and/or Parents, HICP, who have ever cared for an adult or fathers who have ever cared for a child with special needs or Other Fathers who have never cared for a special needs child said that people do not trust them to give care or to parent in a safe and caring manner simply because they are men, compared to only 10 percent of women with the same care responsibilities.
That feeling of mistrust came through clearly in focus groups with men who care for adults. Several reported that people can react to their care work with astonishment and even distrust. Justin said that he often feels “the stares and questions” when he takes his father to his medical appointments, saying “the majority of men that are associated with medical [care] are looked at in a feminine manner.” Roger, 32, who owns his own real estate business in Illinois and who cares for his diabetic grandfather, who lives with him, said people expect him not to be as compassionate and patient as women. “I guess it’s not a typical job for a man to do.”
Mark, who cares for his mother, said “I had an instance on Saturday where we were at the doctor’s office and the receptionist couldn’t believe that I didn’t try to get someone else to bring my mom, so I could stay home and watch football.” Yet Malachi, who cares for his elderly father, said that, at times, he’s met with compassion, but largely because of the surprise of his gender. “Typically women are expected to be in this role,” he said.
In the focus group discussions, some men who care for adults expressed often bitter disappointment in how little support, acknowledgment, or appreciation they often receive.
“I can’t think of any specific support that society currently provides caregivers, other than acknowledging nurses during Nurses Week. Caregivers need more support emotionally and financially. Being a good caregiver usually means you are invested in the wellbeing of the person you are providing care for. This can be rewarding but at the same time mentally draining and can expose you to an emotional roller coaster,” said Mark, who cares for several adults.
When we asked men in the focus groups whether society gives people who provide care, including men, the support they need, the majority said no. Only two said society is doing enough to support those who give care. Six men said people with care responsibilities need more financial support, either making long-term care more affordable, compensating family carers, or paying better wages to paid carers. And three reported wanting more emotional or social support.
“I do not think we as society give other adults the support they need. There was a time in history when it was an honor in American society to take care of the elderly, that got lost somewhere. The way that things are set up now, a lot of families have to both work just to pay bills and don’t have time to caregive. What could be done differently is a universal healthcare system like every other industrialized nation on earth. Further, caregivers that choose to select this as a career should be properly compensated and supervised, I feel that is not the case now,” said Richard, who cares for an elderly neighbor with dementia.
There was a time in history when it was an honor in American society to take care of the elderly, that got lost somewhere.
The Legacy of Cultural Stereotypes and Structural Racism
Large majorities of men (more than 80 percent) across racial and ethnic groups agreed that care work is valuable. White men were more likely than men of color to say that care work is both valuable to society and as valuable as paid work, by five to six percentage points.
At the same time, Latinx respondents were more likely than white respondents to say they lived in families where men do the majority of care—32 percent of Latinx respondents compared to 22 percent of white respondents. (Black respondents, 26 percent, fell in between the other two ethnic groups.) (Figure 14)
What to make of these somewhat perplexing findings that some men of color say they see more men doing the majority of care at home than white men, but value that care slightly less?
Figure 14
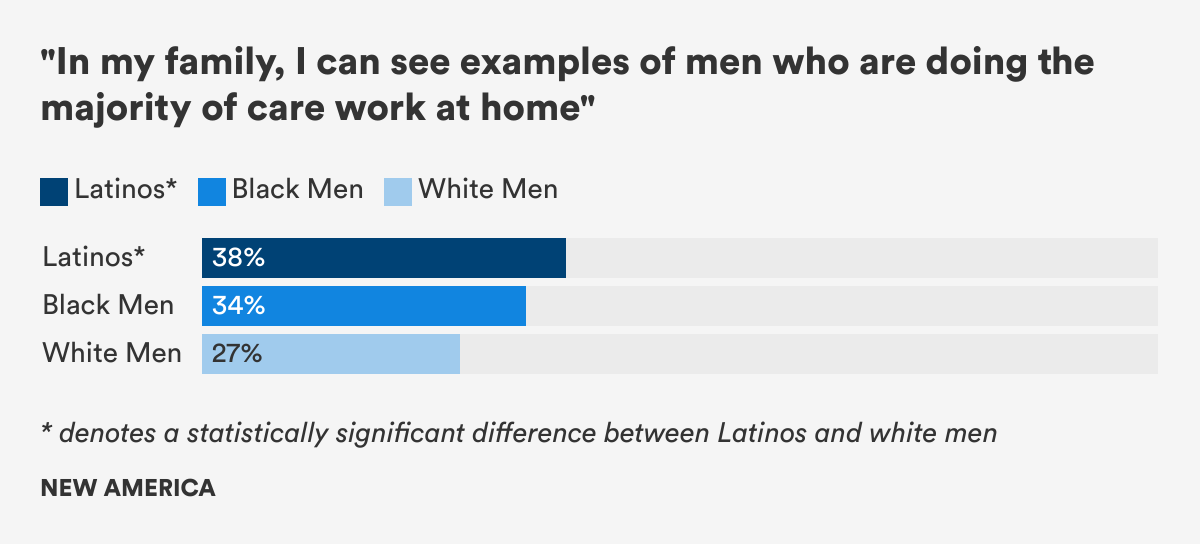
Previous research has found that race, ethnicity, socio-economic status, and other demographic factors play a role in shaping fathers’ attitudes about the value of care and parenting styles. That research found that Black fathers may show less engagement and warmth, but “exert more control and take more responsibility” than white fathers, and that Mexican-American fathers are highly supportive, responsive, engaged, and involved with child care, in contrast to the traditional distant, disciplinarian Latino father stereotype.
Men of color, and Black men, in particular, have long been harder hit by unemployment than white men—the rate is typically about twice as high, particularly in times of economic crisis, putting more men of color in positions to give more care and rely on their partners to provide for the family. It’s too soon to tell how the COVID-19 pandemic will reshape men’s caring role—largely because women, particularly women of color, have been disproportionately impacted, forced out of the workforce by both being overrepresented in the industries most affected by shutdowns and by the closure of schools and childcare facilities. But, if history is any guide, in the years around the 2008 Great Recession, research has shown that while men across race and ethnicity were hard hit by job losses, so were women. Black and Latino fathers’ involvement in childcare increased dramatically, while white fathers’ did not. In the COVID-19 pandemic, communities of color have also been disproportionately hit by the virus itself, meaning that more are being called upon to care for family members.
In an interview, Glen Henry, a Black father of four who documents his fathering experience on his Beleaf in Fatherhood website and YouTube channel, said he was not surprised by the finding that Latino men, in particular, may have more exposure to men who care compared to white men, but that men of color value care slightly less than white men say they do. That perception, he said, may be rooted in the long history of racism in the United States, and how the structural racism built into centuries of slavery and subsequent laws, regulations, and discrimination have made it difficult-to-impossible for Black men to find good jobs with decent wages and benefits in order to be breadwinners, provide for their families and build wealth and stability.
“It’s a role that’s longed for. We’ve longed to be in a position to make money,” Henry said. “But it’s not what we have.” And, he continued, it’s not that Black men don’t value care. Instead, they may see it as a given. “For people who are not privileged, we have to take care of more family members,” he said. “We don’t see it as a burden. It’s more, ‘This is my responsibility as a man.’ I don’t expect to get a pat on my back for taking care of our kids, or helping my aunt pay the rent.”
We don’t see it as a burden. It’s more, ‘This is my responsibility as a man.’ I don’t expect to get a pat on my back for taking care of our kids, or helping my aunt pay the rent.
Ronnie Taylor, the occupational therapist whose experience caring for his infant daughter changed his attitude about care and transformed his life, also said that, for many men of color, providing care may not be a choice. Black people, for instance, are incarcerated at five times the rate of white people, and Latinx people nearly three times the rate as white people, according to the latest data from the U.S. Bureau of Justice Statistics. And the higher unemployment rates for men of color, compared to white men, means that care responsibilities may also be forced out of necessity because the longed-for breadwinning role is unattainable.
“More [Black men] are home with their kids because they can’t go to work. That has a psychological effect on how you value care,” Taylor said. “It’s not your choice. You’re caregiving because someone won’t value you enough to give you a job.”
It’s not your choice. You’re caregiving because someone won’t value you enough to give you a job.
Conclusion
“Women will have achieved true equality when men share with them the responsibility of bringing up the next generation.”
– Ruth Bader Ginsburg in a 2001 address
We set out in this report to better understand men who give care—who they are, what they do, how they think about care, and their experience of care—by comparing High-Intensity Caregivers and/or Parents, HICP, (men who have ever provided care to adults or fathers who have ever cared for a child under 18 with a medical, behavioral or other condition or disability), Other Fathers (who have never cared for a child with such special needs), and men who are Non-Caregivers.
As a reminder, in analyzing our survey data, we found that many people who provide high-intensity care do so in more than one capacity. That is, over half of parents who had ever cared for a child with special needs had also provided care for an adult, and almost a third of those who had ever cared for an adult were also parents who had cared for a child with special needs. Those who fell into one or both of these categories were also more similar than different in the caregiving attitudes measured by our survey. For these reasons, we grouped those who had ever cared for an adult and parents who had ever cared for a child with special needs together as High-Intensity Caregivers and /or Parents, HICP, and compared them to Other Parents—those who have not cared for children with special needs—and to Non-Caregivers. The HICP group warrants further research in its own right, with more detailed measures of attitudes and experience to increase our understanding of how men who care for adults compare to fathers who care for children with special needs, and how these men compare to men who do both types of high-intensity caregiving.
For this report, we initially sought to explore a central question: whether men’s experience of providing care influenced their attitudes about the value of caregiving. We were curious to explore whether men valuing care would be associated with men actually doing more of it.
It’s a critical question. Over the past year, the Better Life Lab’s Men and Care report series, including this one, has found, again and again, a vast disconnect between what men say they want or believe is ideal and what they do. In this report, we found that men overwhelmingly say they value care, that care should be equally shared with women, and that they want to be more engaged and active in care work. But they are unable to embody that ideal of shared care in what they actually do or feel they can do. Understanding what stops men from taking on more care responsibilities and, when they do, what encourages or enables them to continue is key to creating not only more gender equity but better health and wellbeing for people of all genders, children, and families.
We found that men overwhelmingly say they value care, with large majorities saying unpaid care work is just as important as paid work. And yet we found that the belief that care is valuable did not necessarily translate into men taking on more care responsibilities or shape their attitudes about who could or should be responsible for taking those duties on.
Instead, what became clear in analyzing the quantitative, focus group, and interview data is that experience itself is the best teacher. The very experience of providing care can shape men’s attitudes and beliefs and transform men’s lives. Men, contrary to cultural stereotypes, also perform many of the same caring tasks that women do. And men who are High-Intensity Caregivers and/or Parents, HICP, in particular, perform many of the intimate, hands-on tasks, like bathing and dressing, more typically associated with women, and experience more work-life conflict than other men. Employed HICP men report missing work or leaving the workforce entirely because of care responsibilities at the same rate as HICP women.
Focus group discussions held before the COVID-19 pandemic and subsequent interviews after the pandemic hit to capture men’s care experiences in the crisis showed a nuanced picture of gendered beliefs around care. Men who had experience parenting or caregiving were more likely than men in the general population group to say that men, not just women, have a natural instinct to care, that providing care is a skill that can be learned, and that society’s expectations are often what keep men from giving care. Further, when we asked men to share photographs of what came to mind when they thought of the word “caregiver,” men in the general population group thought of nurses or female home health aides caring for the elderly or ill. Men who cared for another adult, in sharp contrast, shared more intimate and immediate photos of themselves and their families.
So the real question, then, is what are the factors that need to change to enable men to have the potentially transformative experience of providing care and living up to their ideal of equally sharing it?
The late Supreme Court Justice Ruth Bader Ginsburg, in her lifelong fight for gender equity, understood that real gender equity for women would only come when workplaces and public policies changed to recognize that all workers have care responsibilities and lives outside of work and require flexibility, schedule control, and support in order to effectively combine work and care. But she also recognized that men would have to change and that the cultural expectations would need to shift for shared care to become an ordinary fact of everyday life. “My plan,” Ginsburg wrote, "would give men encouragement and incentives to share more evenly with women the joys, responsibilities, worries, upsets, and sometimes tedium of raising children from infancy to adulthood. (This, I admit, is the most challenging part of the plan to make concrete and implement.)”
Real gender equity for women would only come when workplaces and public policies changed to recognize that all workers have care responsibilities.
Traditional gendered beliefs that women, not men, are natural carers still have a powerful hold in America. Yet we found that men and their gendered attitudes toward breadwinning and caregiving are not the only nor the greatest obstacle to men being able to equally share care. Instead, structural barriers, too, keep them from embodying the ideal of equal sharing of care that they espouse. For men to share equally in care work, as they say they aspire to, workplaces, public policies, and cultural attitudes are what must change:
- Workplace policies and cultures must change to recognize that all workers, across the gender spectrum, have care responsibilities, not just women. Managers and leaders must provide flexible and remote work options and schedule control. Leaders must rethink and redesign performance management, recruiting, hiring, retention, pay equity, and promotion practices so that these systems no longer disadvantage workers with care responsibilities.
- Family-supportive public policies, including paid family and medical leave, paid sick days, paid annual leave, pay equity, and investments in child and elder care must exist. They must be gender-neutral and must be designed to help all workers combine work and care responsibilities, including men.
- The cultural narrative, unconscious bias, and gendered beliefs that men are providers and women naturally suited to care must continue to shift to recognize, support, and normalize the fact that those with care responsibilities exist across the gender spectrum. This shift is urgent, as elder care demands become more acute as U.S. society ages, and as the child care crisis that the COVID-19 pandemic has made so brutally apparent continues to strain family health, wellbeing, and financial stability and threatens to set gender equity back a generation.
As Ginsburg said, the challenges to overcome to enable men to equally share care are, indeed, immense. But, as our survey, focus group discussions, and interviews with so many men who provide care make clear, so are the rewards.
Methodology
Throughout 2019, the Better Life Lab at New America conducted a multi-modal study of men and care in the United States, with support from the Robert Wood Johnson Foundation and Pivotal Ventures, an investment and incubation company created by Melinda Gates. This research included a quantitative component: a nationally representative survey of 2,966 Americans, in partnership with NORC at the University of Chicago, including oversamples of adult men and fathers of children zero to eight years old. We also conducted five three-day long online discussions using the 20|20 Research’s facilitation platform QualBoard. 20|20 recruited and screened focus group participants for each of the online discussions. The groups were conducted over four weeks in May 2019 and included a total of 68 participants. Participants were compensated for their time. This is part of a larger series of reports on men and care. Click here for more information on survey methodology. And for reports on men and paid leave, engaged fathers and political affiliation and attitudes toward care, visit the Better Life Lab’s Men and Care Project collection page.
More About the Authors

Brigid Schulte
Director, Better Life Lab



