
From Trauma to Development
Abstract
By 2025, children of immigrants will make up nearly one-third of the U.S. child population. More than 94 percent of children of immigrants under the age of six are U.S. citizens, symbolizing a shift in the face of the nation. The ability of young children to learn, grow, and succeed defines what our nation will become, and yet, children of immigrants often lack the necessary resources to grow to their full potential. Additionally, due to a host of factors including their parents’ journeys to the United States, socioeconomic status, citizenship status, language fluency, and the disruptions and destabilizations of the COVID-19 pandemic, the children of immigrants are also coping with trauma that, without proper resources and care, could leave them struggling throughout their whole lives. Relying on interviews with immigrant parents, experts, and advocates in the immigrant and child advocacy spaces, as well as a growing body of early education research, this report summarizes the barriers to learning, growth, and development for young children of immigrants and the policy solutions—like access to early education tailored to their families’ particular needs—that could help them to overcome not only the social, educational, and economic barriers they face, but also to heal from trauma and live happy, healthy lives in the United States.
Acknowledgments
This report would not be possible without the mothers and early education and childcare workers and researchers who shared with me their candid experiences and knowledge. New America's Education Policy Team—particularly, Cara Sklar, Leslie Villegas, and Amaya Garcia—offered critical feedback. I’m also thankful for the support of New America’s Events, Production, Editorial, & Communications team for pushing this report to publication.
Finally and always, I am deeply grateful for the Better Life Lab team and fellows, Brigid Schulte, Haley Swenson, Vicki Shabo, and Rebecca Gale. I am inspired and energized by their brilliance, commitment towards an equitable future, and collaboration. I love dreaming (and scheming) with you all.
Downloads
Executive Summary
There are approximately 18.5 million children of immigrants in the United States. And by 2025, children of immigrants will make up nearly one-third of the nation's child population. More than 94 percent of children of immigrants under the age of six are U.S.1 citizens. The ability of young children to learn, grow, and succeed defines what our nation will become, and yet, children of immigrants often lack the necessary resources to grow to their full potential.
The COVID-19 pandemic revealed and widened racial disparities in society by disproportionately harming historically marginalized groups. Black, Latinx, American Indian/Alaskan Native, and Asian people have had substantially higher rates of infection, hospitalization, and death compared with white people while also being overrepresented in low-wage sectors like retail, service, and care work. As a result, communities of color have disproportionately experienced poverty, hardship, and unemployment during the pandemic. At the same time, the pandemic presented a critical opportunity to reimagine the role of government, which made unprecedented public investments in family-supportive policies such as the Child Tax Credit, food and income supports, expanded unemployment insurance, eviction moratoriums, and paid childcare and paid sick leave to some workers.
Yet these investments have been too little to stop a profound crisis for families with young children and for the early learning sectors, as centers across the nation close their doors and parents of young children exit the workforce or reduce their hours to cope. The Biden administration championed further investments in the form of the budget reconciliation bill, Build Back Better, which notably included childcare, pre-kindergarten, home- and community-based care, paid family and medical leave, and a system for granting work authorization for undocumented immigrants. With no Republican legislators on board and two key Democratic senators against the package, the legislation has been stalled with little hope of advancing since December 2021. The nation must rebuild by reenvisioning governmental roles. This is an opportunity to promote equity in ways that the United States has never seen before, by centering historically alienated and, even villainized, immigrant families.
Meanwhile, the international chaos produced by ongoing wars, genocides, and climate crises continues to produce more refugees, who will bring their children to and have more children in the United States. In late March 2022, the Biden administration announced it would accept 100,000 Ukrainians and offer humanitarian relief to Ukrainians who have been living in the United States without legal documentation since March 1 or earlier as Russia advanced in the south of the country. States across the country are preparing to accept Ukrainian refugees. Similarly in August 2021, when the United States ended its longest war in Afghanistan, over 70,000 Afghans came to the United States on top of the 2.2 million Afghan refugees already in neighboring countries and 3.5 million people forced to flee their homes within Afghanistan's borders.
Drawing from interviews with immigrant families with young children and organizations that serve them, this report highlights their complicated lives and makes social and political suggestions for promoting a fair growing environment for these young children. Seven refugee mothers, who relocated to Tucson, Ariz., were interviewed for this report. The location is limited to where the author lives. About half of the interviews took place in the interviewees’ homes, while the others took place in coffee shops and a McDonald’s depending on the interviewee’s preference. The majority of the interviews included the mother or the mother with her young child(ren), there were two exceptions: Sarqas and her husband Soor Gul Entizar spoke equally together, and Zahra Hasmi conducted the interview with a female friend and her husband present. Hasmi’s husband sat away from us and never spoke, and the friend was there with the hope that I could interview her too. Each interview lasted for about one hour. The interviews were conducted in English or Dari with a translator. The interviewees were compensated with $20 for their time. The money was an acknowledgement of their time. It seems that the interviewees wanted to speak to me with the hope that I could help their circumstances, such as finding a job, enrolling their children in school, finding relatives, or helping their relatives in Afghanistan. Researchers, and organizers of programs across the United States that serve immigrant families were also interviewed by phone or Google Meet. They were not compensated.
The stories in this report are those of people you might unknowingly interact with at various locations, including neighborhood, hotels, grocery stores, etc. Specifically, the report provides an overview of barriers such as family socio-economic status, language accessibility, parents’ educational backgrounds, access to social safety net benefits, and exposure to traumatic events. This report concludes by offering policy recommendations that would boost opportunities for immigrant families and their children. These include a pathway to permanent residency and citizenship, immigrant-friendly social services, work authorization, adult education investments, and critically, childcare programs, including center-based, family, friend and neighbor care, and home visitings, that reach children of immigrants. Some of these strategies have successfully been adapted in communities and states across the United States, and therefore, can be replicated and expanded with adequate investments.
Citations
- The use of the term “American” to describe people from the United States linguistically erases the majority of other Americans. I use United States (U.S.) instead of American to describe people from the United States in an effort to question and resist the imperialistic and U.S.-centric claim to the entire American region.
Justine’s Story
Justine Barawigira’s Tucson, Ariz. apartment is immaculately clean and well decorated. Justine, 26, is a single mother of three children: Joseph, eight, Kingston, four, and Queen Elizabeth, five months, a fact that makes the polished home even more impressive. While we talk, Joseph is still at school, Kingston sits next to me and draws with my pens and notebook, and Queen Elizabeth—truly regal in a white dress and headband—sits happily in Justine’s arms. She just nursed, Justine smiles, when I compliment Queen Elizabeth’s easy nature.
Justine, like many people in the United States and worldwide, lost her job at a cleaning service company at the beginning of the pandemic. She balanced helping Joseph the best she could when schools closed, while caring for Kingston and welcoming her daughter during the pandemic. Prior to the pandemic, Justine held a variety of jobs—working at Target, in hotel housekeeping, and at a computer cleaning service. She does not complain about these jobs, except to say that she is looking for something different, “any job,” she says, especially one with a fixed 8:00am–4:00pm schedule, so she can spend her evenings with her children.
Justine is especially proud of the family she has built because for much of her life, she has been an orphan. Originally from the Democratic Republic of the Congo, her family fled violence and poverty when she was a baby, landing in Uganda. Her father died when she was four years old and her mother died when she was just 11, each from different illnesses. When her mother died, she and her three younger brothers dispersed in different directions “because of life. Our life was hard in Uganda.” Five years ago, UNICEF helped Justine and her then three-year-old Joseph resettle in Arizona.
There is often an expectation that refugees owe the public their stories—to invoke sympathy and to inspire with their remarkable resilience or to convince their audience that they were worthy of refuge in the first place. No doubt, Justine had to narrate her obstacles to UNICEF agents and U.S. officials, who deemed her hardships significant enough to warrant her relocation. Justine does not provide a harrowing account of her youth in Uganda without any family members. Rather than depending on Justine for details when she says, simply, “Our life was hard,” you might imagine your own daughter or sister caring for herself at the age of 11 in Uganda—what dangers might she encounter and what abuses might she endure? Where did she sleep? Which is louder—loneliness or fear—when the sun sets each night?
Contrary to popular belief, the United States does not give money to refugees who resettle here. Instead, the State Department’s Reception and Placement program provides refugees with a loan to travel to the United States, which they are required to repay after they arrive. That money pays for rent, furnishings, food, and clothing, as well as costs of the agency staff case management and other integration services. Like many other refugees, Justine had three months to learn English and immediately started working—the federal framework for refugee resettlement prioritizes rapid employment. She recalls wanting to run back to Uganda during her first year in the United States because the foreignness and loneliness seemed impossible to overcome, a sentiment shared by hundreds of immigrants I have spoken to in my decade-long research on U.S. refugees.
As a single mother, childcare has always been an urgent issue for Justine. Current federal policies do not require resettlement agencies to address the needs of young children in refugee families. As a result, case managers are not trained on early education and care and view caring for young children as a “barrier to employment” to overcome in the resettlement process.
Justine has no choice but to be proactive about finding a solution, “Because I don’t have someone to support me, I need to push myself to do it.” She reached out to the Catholic Charities Community Services that resettled her, and an agent pointed her to “the government on 22nd street” to figure out a childcare alternative on her own. The Arizona Department of Economic Security agreed to subsidize her aunt, also a refugee living in Tucson, to watch her children. The arrangement allows her children to be with a trusted person who cooks familiar food and speaks her native language, flexibility with pickup and drop-off time, and close proximity to home (in the same apartment complex) that eliminates transportation conflicts.
Justine did not want to send her children to a childcare center. “My bus can be late and [the daycare center] can call police and take my child. Yeah, I cannot agree with that.” Indeed, buses can be unreliable in every city and her job can let her out a little late; however, underlying Justine’s decision to not use center-based care is both a cultural preference (many refugees are unfamiliar with early education and care) and a deep need for her children to be with someone she trusts. Additionally, at the root of her fear is a deep mistrust of the U.S. care system to sympathize with her as a Black refugee mother and protect her children.
Her skepticism is well founded. Justine and her children are a part of the fast-changing Black population: one-in-10, approximately 4.6 million Black people living in the United States, were immigrants as of 2019. Black children are far overrepresented in child protection services cases. Additionally young Black children are much more likely to be suspended from preschool than their white peers. People in the United States and around the world have also witnessed the abuse of refugee children by the federal U.S. government, such as separating children from their families and incarcerating toddler children as a strategy to deter fellow migrants and asylum seekers during the Trump administration.
Like the majority of children of immigrants, Justine’s children Kingston and Queen Elizabeth are U.S. citizens by birth. Soon, Joseph will be a naturalized citizen when Justine obtains her U.S. citizenship by passing a naturalization interview and English and civics test. Additionally, their hardships overlap with those of many other children of immigrants, including belonging to a low-income household, having an English-learning parent with limited formal education, and lack of access to good schools. Justine wants Joseph to attend another school because he’s not performing well at his current one; however, she does not know the application process for other schools and transportation would likely be a problem.
Joseph, Kingston, and Queen Elizabeth also experience trauma in addition to these material challenges. The word “trauma”—a term foreign to many immigrant tongues that instead say war, poverty, genocide, displacement, death, family separation—never comes up during our conversation. Justine names her memory as “too busy” and depends on her children to “make my memory different” and “clean [my] memory.” When asked about her hopes for her children, Justine pauses before answering, “You know, like, because I don't have any family. I'm happy to say that ‘This is my family.’ I'm being with my family, you know? Yeah. Because I don't have anybody. Now I'm happy sometimes from inside when I … think about them. When I'm talking with my kids, they make me to be happy. They make me without thinking wrong things. A lot of things. You know, they make me to be happy every time because I'm seeing them every time because they're my family.”
Although Justine does not elaborate on the “wrong things,” what is clear and significant is that her children play a critical role in helping Justine heal from her past trauma. Shouldering the burden of standing in for the family that Justine lost at a young age is tremendous pressure that her children must negotiate. Even if Justine does not tell her children about her trauma, her children experience her painful past—a phenomenon known as intergenerational trauma or post-memory. That is, the trauma that children of immigrants face is unique. In addition to the many barriers they face, the intergenerational trauma results in guilt and unmanageable pressure to succeed in a new country in order to make all the sacrifices and sufferings of the parental generation worthwhile. Many children of immigrants feel that their own struggles are not legitimate compared to their parents’ obstacles.
Moreover, as psychotherapist Resmaa Menakem explains, trauma may be passed down through parents’ actions and even DNA. Pediatrician Nadine Burke-Harris makes the comparison of the effect of trauma poisoning children’s brains to the exposure of lead. There are opportunities to help these children overcome this trauma, including evidence-based therapies like biofeedback and mindfulness and case management to help families get the resources that they need to overcome their circumstances and prevent children from being exposed to more categories of traumatic experiences.
Early childhood trauma has been associated with reduced size of the brain cortex, which is responsible for many complex functions including memory, attention, perceptual awareness, thinking, language, and consciousness. As a result, early recognition and interventions on childhood trauma is equally important to investments in tangible programs, such as housing, health and food services. Early education and care programs, where children spend extensive time, have the potential to intervene in the healing of the whole family.
There are millions of families like Justine’s in the United States, and promoting a more equal environment for them to thrive requires connections among organizations working on immigrant justice, racial justice, family justice, labor justice, and child welfare justice. This report provides a profile of young children of immigrants and an overview of the obstacles they face, many of which are the same struggles Justine’s family encounters. The paper names strategies to mitigate these challenges and aims to inform efforts to rebuild a more equitable way of life post COVID-19 pandemic that truly works for all children and their families. In addition to policy reforms, this report also aims to promote intimate changes in how early education teachers, case workers, doctors, neighbors, and friends interact with immigrant families, particularly with the children of immigrants. Individual compassion and vote, after all, underline democracy.
The Changing Faces of the United States
The significance of the immigrant population in society cannot be overstated nor ignored as even at reduced levels, immigration made up a majority of population growth in 2021. This population includes lawful permanent residents, those with temporary visas, refugees and asylum seekers, and unauthorized immigrants. The immigrant population live myriad lives with disparate income, education, citizenship status, and English proficiency. While some immigrant parents are among the most educated people, others have low levels of education and work in sectors of the U.S. labor market relying on low-skilled workers, such as agriculture, service industries, and construction. They speak hundreds of languages, making sufficient translation and interpretation a challenge in every service.
States in the Southeast, Midwest, and West have all seen very rapid growth in their foreign-born populations. The population of young children of immigrants in North Carolina, Nebraska, and Arkansas grew 270 percent, 269 percent, and 244 percent, respectively, between 1990 and 2000. The dispersal of immigrant families across the country means that issues related to their health, well-being, education, and integration are new to many communities. This means that newer destination states might not have the necessary infrastructure to support these children and their families. For example, between 2016–18, internal migration may have played a role in the rise in children’s uninsured rates as immigrant families relocate from top destination states like California and New York to the Southeast and Midwest states. Additionally, states’ social and political views on immigration can affect immigrant families’ use of public programs. For instance, immigrant families in states with more generous public policies for immigrants were more likely to use Head Start and public pre-kindergarten than parental care.
The Young Children of Immigrants
The United States has become the first high-income country in the world with a majority-minority child population. From 2006 to 2019, the share of children of immigrants increased from 22 to 25 percent of the total child population, and by 2025, children of immigrants are expected to represent nearly one-third of the U.S. child population. Almost all—94 percent—of young children of immigrants are U.S.-born, and most live in mixed-status families with one or more noncitizen parents; 29 percent of young children of immigrants have undocumented parents. Latinx and Asian Americans and Pacific Islanders predominated among the country’s immigrant parents of young children, 50 and 26 percent respectively, between 2014–18. And a majority—60 percent—of children of immigrants live in six states that are traditional immigrant destinations (California, New York, New Jersey, Florida, Illinois, and Texas).

This report prioritizes the majority of children of immigrants. They grow up in particularly vulnerable circumstances, facing disproportionately high rates of poverty, low parental education, linguistic isolation, and especially exposed in the wake of the COVID-19 pandemic—all factors associated with low performance in school. Their exposure to these obstacles results from experiences of war, genocide, climate crisis, gang violence, and/or other external circumstances that pushed them out of their homeland and the structural inequalities in the United States. In other words, the challenges immigrant families experience are not personal barriers. As a result, promoting the wellbeing of children of immigrants requires systematic changes rather than demanding immigrant families to overcome hardships on their own.
Children of Immigrants and the COVID-19 Pandemic
The COVID-19 pandemic has had profound detrimental effects on children of immigrants. More than 75 percent of children dying from COVID-19 are minorities, echoing the disproportionate death rates among adults. The disproportionate representation of minority deaths may result from, among other things, mistrust of health services and the rise in children’s uninsured rates. Beginning in 2016, the uninsured rate among Latinx children with only foreign-born parents rose, resulting in roughly 515,000 more children who were uninsured in 2018 than in 2016. The parents’ undocumented status negatively affected their children’s development and wellbeing. In 2018, the uninsured rate for Latinx children with only foreign-born parents was 3.4 times higher than the rate for non-Latinx white children and 2.5 times higher than the rate among Latinx children with at least one U.S.-born parent.
Immigrant families faced higher rates of COVID-19 in their communities due to social disparities, such as wealth and education gaps. Other conditions that put immigrant families at higher risk include: overcrowded housing; lack of access to medical care, insurance, and sick leave; disparities in testing, infection, and hospitalization; food insecurity; pre-existing conditions; parents who are essential workers and cannot work from home; and unsafe working conditions, especially for migrant farmworkers. For immigrant families with members who were able to keep their job, many of them hold low-wage jobs considered essential, which don’t always offer employee-sponsored health care or paid sick leave. With an increased risk of exposure, lack of health insurance, and fear of accessing health care services, there are concerns that some immigrants might not seek testing or wait too long to receive care. Voice of San Diego, a nonprofit news organization, found that immigrants account for more than half of the people who died from COVID-19 in San Diego County in the first year of the pandemic, even though they make up 23 percent of San Diego County’s population.
Behind these shocking disparities are the ones left behind–orphans. According to the Centers for Disease Control and Prevention, more than 140,000 children under age 18 in the United States–from April 1, 2020 through June 30, 2021—lost a parent, custodial grandparent, or grandparent caregiver who provided the child’s home and basic needs. One U.S. child loses a parent or caregiver for every four COVID-19-associated deaths, a new modeling study published in Pediatrics reveals. Children of racial and ethnic minorities accounted for 65 percent of those who lost a primary caregiver.
American Indian/Alaska Native children were 4.5 times more likely to lose a parent or grandparent caregiver than white children, Black children were 2.4 times more likely, and Latinx children were 1.8 times more likely compared to white children. While the data were not separated by immigration status, we can expect that children of immigrants are disproportionately impacted since other data shows that immigrant families accounted for higher rates of the virus. The loss of a parent has adverse effects on children, including mental health problems, shorter schooling, lower self-esteem, sexual risk behaviors, and increased risk of substance abuse, suicide, violence, sexual abuse, and exploitation.
Child poverty rose between 2018 and 2020 for Black and Latinx children. A report reveals that Latinx child poverty rose from 2019 to 2020, during the COVID-19 pandemic, despite the unprecedented public investment in family-supportive policies. As with the rates of uninsured, the rates of increased poverty differ by parents’ citizenship statuses: 6.1 percentage points among Latinx children living in families headed by non-U.S. citizens (including both authorized and unauthorized immigrants); 4.9 percentage points among families headed by naturalized U.S. citizens; and 3.0 percentage points among families headed by U.S.-born citizens.
The increase is particularly troubling because the poverty rates among Latinx children were already high; in 2019 the poverty rate was 36.3 percent among families headed by non-U.S. citizens. The poverty rates are disproportionately high among immigrant families. Half of immigrant parents with children ages 0–4 are low-income, and 30 percent of them are working poor, employed with an annual family income of below 200 percent of the federal poverty level. Immigrant families are more likely to work a substantial number of hours more than families of children with U.S.-born parents; however, these families are more likely to have low incomes. The majority (54 percent) of immigrant parents of children ages 0–4 work in low-skilled jobs.
Unlike U.S.-born families, many immigrant families, who lost their job or had their hours reduced, did not qualify for most forms of federal aid, such as unemployment or recovery rebates, to help make up for the lost income. They also didn’t qualify for federal public benefit programs like Supplemental Nutrition Assistance Program (SNAP), regular Medicaid, Supplemental Security Income, or Temporary Assistance for Needy Families.
While U.S. citizen children in immigrant families can receive federal benefits if they meet the eligibility requirements, many families are afraid to access these or any other type of service due to the Personal Responsibility and Work Opportunity Reconciliation Act of 1996 and the Public Charge Final Rule that went into effect on February 24, 2020. This rule expanded the criteria that the government can consider whether a green card and temporary visa applicant is likely to become primarily dependent on government assistance, making it more difficult for some immigrants to obtain lawful permanent residence if they access certain public benefits like food stamps and housing vouchers. Although the Biden administration restored the public charge rule to the status quo before the 2020 change, the public charge rule still applies to receipt of Temporary Assistance for Needy Families and Supplemental Security Income, programs that supplement families’ income and reduce poverty. The Immigration and Nationality Act requires officials to take into account whether a prospective immigrant could become a public charge, without explicitly defining the term. That is, the language around public charge remains vague and up to the discretion of officials. According to Shelby Gonzales, vice president for immigration policy at the Center on Budget and Policy Priorities, immigrant families continue to forgo critical resources.
Research indicates the “chilling” of such rules, whereby immigrant families avoided public programs out of fear of immigration-related consequences, were widespread even before implementation. One in five adults in immigrant families with children reported chilling effects on public benefit receipt in 2019. Families withdrew from benefits regarding food, housing, medical care, and disaster relief—all of which are critical to the wellbeing of their children. Immigration experts estimate millions of children in immigrant families could be affected, many of whom are U.S. citizens, including documented immigrants who withdraw from programs because of confusion about the new rules. Additionally, the local implementation of section 287(g) of the Immigration and Nationality Act and the Secure Communities program, which authorizes local law enforcement agencies to enforce federal immigration laws, produced profound mistrust of health services among Latinx persons, leading them to avoid health services and sacrifice their health and the health of their family members.
A Children’s Defense Fund-Texas report found that between December 2017 and April 2019, Texas experienced a precipitous drop in enrollment in benefit programs: SNAP lost 520,000 of its enrollees, a drop of 13.5 percent. Women, Infants and Children (WIC) lost 155,726 enrollees, or 18.8 percent of its caseload. Immigrant families across Texas began to withdraw their citizen and lawfully-present children from Medicaid and Children's Health Insurance Program (CHIP) in addition to food assistance. VELA, which provides assistance, support, and training to families who have children with disabilities in Austin, Texas, found that 80 percent fewer VELA families were enrolled in SNAP, between 2019 and 2018. Foundation Communities, an organization in Austin that offers health insurance enrollment assistance (among other programs) revealed that in 2018 during the open enrollment for the Affordable Care Act health insurance marketplace, they had seen a 16.9 percent reduction in immigrant clients, compared with only a 5.4 percent reduction in nonimmigrant clients, from their 2017 open enrollment numbers. Epiphany Community Health Outreach Services, a non-profit organization in Houston that connects low-income, largely immigrant clients with health, social and educational resources, saw a 42 percent reduction in Children’s Medicaid enrollments, a 42 percent reduction in adult Medicaid and CHIP-Perinatal services, and a 37 percent decrease in SNAP enrollments, between 2016 and 2019.
Nationally, 11.4 percent of immigrants with children reported that they or a family member avoided a nutrition program (SNAP or WIC) in 2019. In terms of access to health care, more than 1 in 4 children of immigrants did not have health insurance in 2019 (25.5 percent compared to 5.1 percent of native-born citizen children). Despite a federal directive ordering states not to withhold childcare subsidies from U.S. citizen children with undocumented parents, some are, at a minimum, tacitly unhelpful or unwelcoming. The state of Utah, for instance, asked applicants whether they are legally permitted to work in the United States when the state was pressured to stop checking citizenship to decide who gets benefits. By extension, Utah effectively found a way to continuing to deny children of immigrants, U.S. citizens, access to federal safety net programs like Medicare, SNAP, and CHIP. And though the government has specified that COVID-19-related care will not be used as part of public charge considerations, immigrants are not seeking medical care related to the COVID-19 out of fear of consequences for their immigration applications or fear of deportation, according to immigrant advocates and medical personnel.
The recent increase in uninsured and poverty rates leaves children especially vulnerable during the pandemic. It is particularly concerning that the uptick was limited to the one of the groups hardest hit by COVID-19, Latinx children with foreign-born parents. The social safety-net programs effectively penalize the 3.5 million children who have mixed-status families. Unemployment benefits require sufficient formal earnings as an eligibility criterion, which may be difficult to meet for many Latinx workers in low-wage or seasonal jobs. Additionally, many programs impose immigration restrictions by requiring Social Security numbers for all family members or by banning public assistance to most non-citizens through the 1996 welfare reform law. Responding to the pandemic’s impact on immigrant families, one year after, recent Economic Impact (stimulus) Payments and the temporary Child Tax Credit expansion have allowed immigrant families to access benefits for their U.S. citizen children by making individuals and children, rather than the family, the basis of eligibility. The ability of this change to reduce the adversity faced by immigrant families in poverty requires increasing awareness and combating distrust of government in their communities.
In addition to the barriers to access nutrition and health programs, immigrant parents do not have criteria, such as high formal education and English-proficiency, to financially advance and help their children with school. Immigrant parents of children ages 0 to 4 are four times less likely to hold a high school diploma or equivalent than their U.S.-born counterparts. Although they represent only one-quarter of the total population of parents, 57 percent of parents of children ages 0–4 without a high school diploma were immigrants. Significant shares of immigrant parents had less than a ninth-grade education: 15 percent of those with children ages 0–4 compared to 1 percent of U.S.-born parents.
About half of immigrant parents of young and elementary-school age children are English learners. Many immigrant parents experience the compounded impacts of poverty, low education, and being English learners. One-third of immigrant parents of young children were both low income and English learners. Low-income immigrant parents are three times more likely to lack a high school diploma/equivalent than low-income native-born parents. Because mobility in the United States usually requires education prerequisites of high school diploma/equivalent and English proficiencies, many immigrant parents with young children become stuck in low-wage jobs that offer little room for autonomy and advancement.
While the majority of immigrant parents are employed, parents not in the labor force tend to have a low level of education attainment, which heightens their isolation and alienation in the United States. Zahra Hasmi, a 41-year-old from Afghanistan who has lived in the United States for three years, is illiterate in all languages and describes helplessness in many aspects of her life. Her five-year-old daughter recently started school when Zahra learned about the school from a friend. She does not know the name of the school nor if it’s kindergarten or preschool. In fact, she is also unsure of her daughter’s age—she presented her daughter’s green card to the school and trusts that the school will place her daughter in an appropriate class. In addition to her illiteracy, for the majority of her motherhood, her biggest concern has been whether her children will return home alive or dead.
Murders of her family dominate her mind and determined many of her life events. After her father and uncle were burned alive in front of her, she married a man who worked for the U.S. embassy. She doesn't know how old she was when she got married; she only knows that marriage might help her stay alive. Four of her cousins were also burned alive in their house; her mother still carries a bullet left by a member of the Taliban. She bookends the interview with questions on how to help her family escape Afghanistan, suggesting feelings of responsibility and guilt. Zahra’s uncertainty, feelings of helplessness, witnessing of atrocities against her family members, and prolonged sadness have a cumulative effect on the family and the parent-child relationship.
Trauma’s Impact on Young Children
Justine’s and Zahra’s stories reveal the prevalence of deaths: the destruction of communities and families among refugees. This report uses the term “trauma,” following the growing awareness of its impacts on young children among civilians and policymakers, despite the risk of "psychiatric universalism." Trauma among young children is defined as “an actual or perceived danger that undermines a child’s sense of physical or emotional safety or poses a threat to the safety of the child’s parents or caregivers, overwhelms their coping ability, and impacts their functioning and development.”
Trauma cannot be isolated as the malfunction of the mind and removed from cultural and regional specificities; trauma is rooted in geopolitics, race, gender, and economic disparity. Living under poverty and other structural inequalities impacts young children’s development with lifelong consequences. Young children who live in poverty are more vulnerable to negative effects of trauma than are children living in higher-income families. According to child development scholar Hirok Yoshikawa, disastrous work conditions–including low wages and job duties that come with little opportunity for self-direction or autonomy—and lower access to center-based childcare lead to lower scores on measures of vocabulary, motor, and perceptual skills in children at 36 months.
Contrary to popular belief that young children are immune to traumatic situations, they are actually experiencing the most severe of consequences and are the most vulnerable to long-term negative effects of trauma. Trauma during the early years can damage the cortex, the hippocampus, and the amygdala of the brain. Children as young as three-months-old have demonstrated post-traumatic stress symptoms. Trauma disrupts healthy development by interfering with a child’s ability to develop positive relationships with adults and peers, to learn and play, and to self-regulate their emotions, attention, and behavior.
In addition to structural barriers, young children of immigrants—particularly refugees—are more likely than their peers to experience trauma due to experiences before, during, and after migration, particularly due to exposure to violence and separation from family members. Young children of immigrants experience a range of violence, including wars and genocides directly or through their parents and caretakers, being a product of rape, family separation, being raised by mothers who were blinded by witnessing atrocities, or witnessing the shooting of one’s parents as toddlers by a police officer. There has been recent development to recognize these particular obstacles experienced by children of immigrants. The original landmark research on adverse childhood experiences—events related to abuse, neglect, and household challenges of parental separation, substance abuse, incarceration, violence, and mental illness—overlooked children of immigrants because they focus on conditions inside the home rather than community or outside actors. The updated survey includes: racism, witnessing violence outside the home, bullying, losing a parent to deportation, living in an unsafe neighborhood, involvement with the foster care system, experiencing homelessness, living in a war zone, witnessing a family member being abused, involvement with the criminal justice system, and attending a school that enforces a zero-tolerance discipline policy. Children of immigrants can be impacted by the trauma experienced by members of their community even if their own family was not directly affected—a phenomenon called historical trauma. Historical trauma leads many members of the community to feel a pervasive sense of hopelessness. Moreover, the trauma of children of immigrants often continues in the United States from discrimination and bullying, problems in school, and struggles with their own or family members’ acculturation.
Language and cultural barriers can prevent caretakers, teachers, and other staff from helping young children. Furthermore, immigrant and refugee families are less likely to access early education services that can be a touchpoint for other supports. In general, immigrant populations are less likely to seek mental health services due to the lack of language access and culturally relevant services, financial burden, and cultural stigmas around mental health. Asian Americans are three times less likely to seek mental health services than are white Americans. Only 22 percent of Latinx Americans and 25 percent of Black Americans received care among a survey of people with diagnosed need for mental health care. Trauma can become normalized within a community that has been through shared violence—everyone has nightmares, everyone has insomnia, everyone is sad—decreasing the likelihood of seeking treatment. Additionally, the Western framework of mental illness might not be culturally appropriate. Others simply might not know about the various resources available.
The parents’ citizenship status has a tremendous impact on their young children’s mental health: Children living with unauthorized parents are more likely than their peers with parents who are U.S. born or legal immigrants to experience psychological distress and economic instability, factors tied to negative child development. Additionally, maternal depression—widespread among low-income mothers—has been linked to negative impact on young children’s cognitive, socioemotional, and behavioral development. Excessive maternal stress can negatively affect genetic programming during fetal development, leading to undesirable birth outcomes, such as preterm births and low birth weight. Infants born to women who experienced four or more childhood adversities were two to five times more likely to have poor physical and emotional health outcomes by 18 months of age.
Policy debates, often times dehumanizing, about undocumented immigrants fail to consider the effects on the children of policies targeting the undocumented. Contemporary immigration actions and rhetoric have had profound and far-reaching adverse impacts on immigrant parents and their children. Specifically, the Trump administration’s immigration policy shifted the way large numbers of families, including many U.S. citizen children, understand and live their lives. Since late 2016, doctors and service providers report having seen more children exhibiting stress- and anxiety-related behavioral changes, including symptoms of toxic stress, due to fear that a family member will be deported.
The American Academy of Pediatrics expressed concerns for the development of children’s bodies and brains due to exposure to prolonged, unmitigated anxiety that their parents will be taken into custody or deported. Toxic stress produces damaging effects on learning, behavior, and health across the lifespan. The research demonstrates that more adverse experiences in childhood leads to greater likelihood of developmental delays and later health problems, including heart disease, diabetes, substance abuse, and depression. Toxic stress disrupts children’s brain architecture and affects their short- and long-term health, which is particularly critical during the first two years of life when rapid brain development occurs, according to Julie Linton, a co-chair of the American Academy of Pediatrics’s immigrant-health special-interest group.
Not only is trauma especially prevalent in early childhood, infants and toddlers cannot verbalize their feelings, talk about frightening events, or describe their nightmares. As a result, toddlers might express toxic stress through temper tantrums, learning problems, memory issues, going to the bathroom, or having trouble eating or sleeping. Even before birth, immigration enforcement has been shown to put children’s health at risk. Premature and underweight births—complications that put babies at risk for infant death or long-term health problems—were shown to be connected with the 2008 worksite raid in Postville, Iowa (the largest single-site immigration raid in U.S. history): babies born to Latinx mothers in Iowa within 37 weeks of the raid were 24 percent more likely to be underweight compared to births over the same amount of time one year earlier. This increased risk was not found in babies born to non-Latinx white mothers in Iowa.
Intensified anti-immigration policies and rhetoric, particularly in the four years of the Trump administration, produced anxiety across the entire vastly diverse immigrant population regardless of their immigration status. A George Washington University study of 213 Latinx parents of adolescent children echoes the heightened fear. Among the surveyed participants, 80 percent worried about family separation; 70 percent struggled to imagine being in a better job or making more money; 60 percent worried it would be hard for their child to get a job; and 58 percent worried it would be hard for their child to finish school. That is, immigrant parents, regardless of their status, expressed anxiety about their daily existence, family unity, and their children’s future in the United States. Even parents of U.S. citizen children were just as likely to worry about their children’s opportunities to finish school and to warn their children to stay away from authorities as parents of noncitizens. The researchers add that parents’ psychological distress harms their children: “adolescents whose parents are depressed and/or anxious face heightened risk of poor social functioning, academic failure, and mental health problems.”
Early Education and Care as a Path Towards Equity
Young children of immigrants lost access to many critical interventions beyond daily lesson plans. For the children of immigrants, the impacts of COVID-19 on childcare and education are compounded by structural inequalities that long preceded the pandemic. Distance learning prevents teachers from engaging with undocumented students’ trauma and anxieties. Immigrant students additionally cannot access hot meals and caring adults, including teachers, school counselors, and nurses, who might be able to mitigate their losses and challenges.
Extensive studies in economics, neuroscience, medicine and developmental psychology all conclude that early childhood investments can benefit children, parents, and nations because early childhood, beginning in infancy, allows profound opportunities to advance children’s skills in reasoning, language acquisition, and problem solving. Public investments in early childhood education bring substantial returns in children’s educational trajectories and a more skilled future workforce because early education improves children’s educational performance and attainment, improves health, decreases crime, and improves long-term economic self-sufficiency and returns.
The importance of early education is widely recognized internationally. According to the United Nations Educational, Scientific and Cultural Organization, early childhood care and education “is one of the best investments a country can make to promote human resource development, gender equality and social cohesion, and to reduce the costs for later remedial programmes. For disadvantaged children, [early childhood care and education] plays an important role in compensating for the disadvantages in the family and combating educational inequalities.”
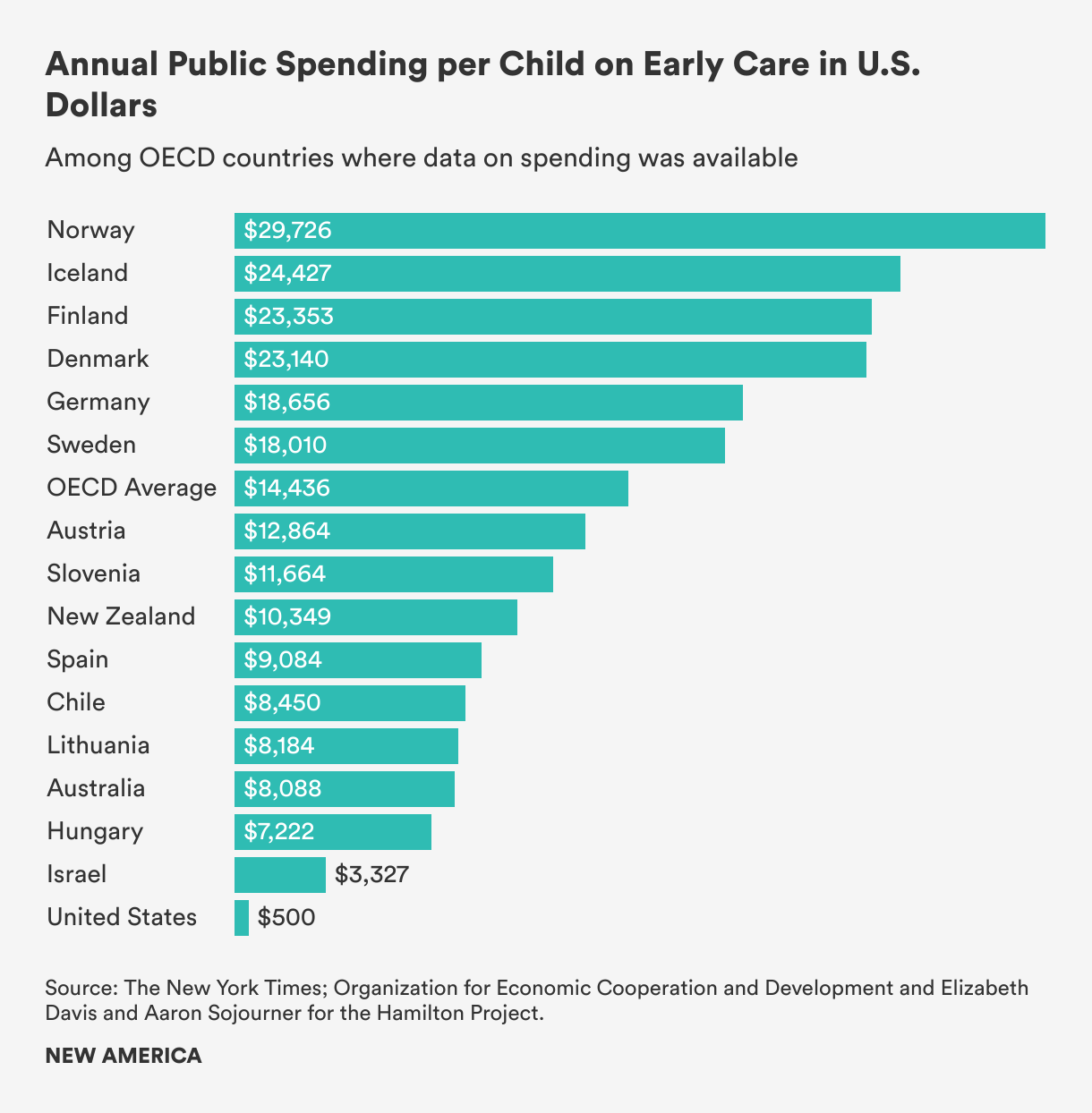
Despite the research on the dramatic development of children in the first few months and years of life, the United States lags significantly in investment in young children’s education and care compared to other wealthy nations. The New York Times shows that the United States spends less than 0.2 percent of its GDP (gross domestic product) on childcare for children two and under—which amounts to about $200 a year for most families, in the form of a once-a-year tax credit for parents who pay for care—while other wealthy countries in the Organization for Economic Cooperation and Development spend an average of 0.7 percent of GDP on toddlers, mainly through heavily subsidized childcare.
Access to early education is unequal. Differences in access to and utilization of early care and education programs depend significantly on income and educational attainment of the parents. Participation in early childhood education is high among children from highly-educated and high-income families. Since the 1970s, children of less-educated mothers are still less likely to attend preschool. In the United States, 90 percent of families in the top 20 percent of income distribution are already purchasing preschool education for their children. In contrast, among families in the lowest 40 percent of income distribution, fewer than 60 percent of children are enrolled in preschool education. Families below the federal poverty level paid an average of 30 percent of their income in childcare costs compared to 8 percent among non-poor families. This inequity produces gaps in cognitive, linguistic, social, and emotional skills that become evident well before children enter kindergarten.
For years, early childhood education has been recognized as a meaningful avenue to compensate for the disadvantages in the family and reduce educational inequalities. In addition to promoting the development of children, quality and sustained care can help immigrants’ children adapt to a new socio-cultural environment, mitigate the impact of trauma, and offer critical wraparound services. Learning environments attentive to safety and trust through consistent routines and expectations can restore a child’s feelings of control after adverse experience.
Early Head Start, a federal program launched in 1996, provides services for at-risk pregnant women, new mothers, children ages zero to three, and their families, and focuses on positive parenting and home environments and children’s developmental outcomes, has shown positive results for cognitive development and language acquisition. Children who participated in Early Head Start showed less aggressive behavior, greater vocabulary and language development, and higher cognitive skills upon the program’s completion, and parents who received Early Head Start services showed greater engagement during play and greater support for language and learning development at home. Head Start, which serves low-income three- and four-year-olds, improves educational outcomes (increasing the probability that participants graduate high school, attend college, and receive a post-secondary degree or certificate) and promotes social, emotional, and behavioral development (adulthood measures of self-control, self-esteem, and positive parenting practices).
Attendance in early education programs in general, and Head Start in particular, has been shown to raise reading and math test scores for children of immigrants. Head Start participation also increases positive parenting practices for each ethnic group and for participants whose mothers did not have a high school diploma or equivalent when compared with the outcomes of children who went to a preschool other than Head Start. In addition to offering early childhood development services, Head Start programs provide comprehensive assessment and services for the whole family, including education, nutrition, and health/mental health care, and even employment of some refugee parents by Head Start agencies.
Barriers to Early Learning and Care for Children of Immigrants
Like Justine’s and Zahra’s families, the majority of children of immigrants do not use center-based childcare, despite the well-documented benefits of early learning services on children’s school readiness and long-term cognitive, socioemotional, and educational outcomes. The majority (53 percent) of children of immigrants under six receive childcare from parents. Only 17 percent of children of immigrants are in center-based care. The use of center-based care is lowest among immigrant parents with less than an eighth-grade education, as compared with approximately 60 percent of the general population. These children are also less likely to attend preschool and Head Start programs.
There are a number of reasons why immigrant families enroll less in early childhood education overall. Some of these reasons are the same as those faced by all parents: costs, waiting lists, locations, service hours that do not cover the full workday, and lack of information about available programs. As mentioned above, immigrant parents are more likely to have low incomes and nonstandard work hours than U.S.-born parents, and thus, especially affected by schedules. Because transportation is a major issue as many rely on public transportation, location becomes another difficult calculus of scheduling. Poor immigrants tend to live in segregated neighborhoods with fewer childcare services. Children who live in areas with the highest share of foreign-born parents are about 13 percent more likely to live in a childcare desert than those who live in areas with the lowest share of foreign-born parents. In addition, immigrant workers are 15.7 percent more likely to work during nontraditional hours and 25.2 percent more likely to work weekends compared to similarly situated U.S.-born workers. Only 8 percent of childcare centers are open during these times, making family, friend, and neighbor (FFN) care—also referred to as kith and kin care, relative care, informal care, home-based care, and license-exempt care—all the more essential for immigrant families.
Obstacles such as parents’ language barriers, logistical barriers to enrollment, and lack of comfort with available programs can all prevent immigrant families from enrolling their children in early education programs. A study on 2,500 immigrant families found that families relying on parent care were less proficient English speakers, less educated, earned less money, and had mothers who worked less. Maternal employment predicted home-based care usage much more strongly than the availability of care centers, suggesting either a preference for home-based care over center care that is unique to immigrant families or that the likelihood of performing low-skill work makes center-based care less accessible due to its cost and inflexibility of schedule. This study also shows that the decreased availability of non-English speaking childcare providers increased the probability of parent care. The decrease in the availability of non-English speaking providers within 20 miles of families’ homes lowered the probability that children would experience home care, center care, or Head Start versus parent care by 35 percent, emphasizing the significance of language continuity in the choice of early education and care.
Like Zahra Hasmi, many refugee families are isolated from the general population, and therefore, do not know about early education options. Furthermore, the violence in their home country produces anxiety around separation from their young ones. Zahra Mohammed, 22, who has been in the United States for about a year, states that her three-year-old daughter is too young to leave her care. She adds that she might let her daughter attend preschool after she learns "American rules." Mohammed’s unease about preschool became further explained when her mother expressed worries about the possibility of Mohammed being kidnapped when the interview ran a little over an hour. Bibi Abdullah, 26, who has been in the United States for five years, describes the belief that she is safe as the most difficult adjustment in the United States. On one occasion, she ran a red light and sped off because she was so certain that the car behind was following her. She didn’t notice the police siren chasing her until one officer came at her from the front. She recalls sleeping a few hours at night, holding tightly onto her daughter and showing up at her daughter’s school to check on her safety. Bibi said it took her over a year and interactions with many supportive people to let her guard down.
Furthermore, many immigrant parents express fear around center-based care. They worry that child rearing practices, which may be historically rooted and culturally normative, may place them in vulnerable positions in the United States where they may not be viewed as acceptable. They also worry about being tracked, monitored, or reported. Additionally, deep-seated fears for some around legal status increase hesitance to engage in services. The immigration status of family members influence use of Head Start and Child Care and Development Block Grant, even though Head Start has no citizenship restrictions and the Child Care and Development Block Grant funding is exempt from verifying the immigration status eligibility of any child. The Child Care Development Fund is a federal and state partnership that provides childcare assistance, in the form of subsidies, to low-income, working families with children under age 13. These subsidies help low-income families to access early education and care for their children and support parental work or participation in education and training activities. While the grant regulations make it clear that childcare subsidies target children, and therefore that their parents’ immigration status cannot be considered in qualifying, of the 13 states that contain 80 percent of the Latinx population, 12 requested the Social Security numbers for household members in Child Care and Development Block Grant applications, and seven of these states did not indicate that providing the Social Security numbers was optional. The lack of clarity can deter immigrant families from applying even though their children qualify.
Local context around immigration and parents’ prior experiences with other government programs can affect the relationship between parents and early childhood education providers. For example, immigrants may have interactions with public officials that lead to mistrust of government institutions, including school-based pre-kindergarten programs, particularly in cities where new immigration enforcement laws are passed.
Making Early Education and Care Accessible
Because center-based care and Head Start have shown to benefit preschool-age children and prepare them for school, both psychologically and scholastically, the underutilization of publicly funded early education programs by immigrant families is troubling. Access to high-quality early childhood education and care is critical for minority and low-income children, who are often at greatest risk of falling behind. Compared with children with U.S.-born parents, children of immigrants begin school, on average, with fewer of the early literary, numerical, and language skills that support future academic success. The children who need sustained and quality childcare the most in order to break systematic barriers, such as low-income, limited English proficiency, and low-education, do not have access to it.
As mentioned above, the potential of universal pre-kindergarten and expansion of quality and affordable childcare benefit will not reach children of immigrants if policies fail to address the many reasons that prevent immigrants from using childcare programs: English language and literary barriers, the fear of being a “public charge,” concerns of racism and cultural bias, transportation, cultural responsiveness, and non-traditional hours. Publicly funded centers that continue to reflect a white dominant standard of quality without addressing lack of racial diversity, institutional racism, language barriers, and shortage of cultural brokers will alienate immigrant families.
In addition to mitigating structural barriers, including language access, scheduling, location, transportation, and cost—factors that shrink initial enrollment and continued attendance among many immigrant families—programs can simplify enrollment, initiate cultural aware outreach, advance staff recruitment and ongoing training, and develop trusting relationships with parents in order to reach more immigrant families. All of these suggestions have been successfully carried out and can be adapted nationally with adequate funding and initiatives.
Data Collection
The first step in connecting immigrant families to early learning programs is to learn who the immigrant families are in a community, where they are, the extent to which they enroll in early education programs, and the issues they face that affect their willingness to access these programs. All Head Start grantees are required to conduct community needs assessment every three years to determine the demographic makeup of eligible families and kids, including their numbers, geographic locations, and racial and ethnic compositions. These assessments also study local concerns and community resources to identify and prioritize families most in need. Like Head Start, Washington state requires local pre-kindergarten programs to conduct community needs assessments every three years. Providers are asked to calculate the number of children by race and ethnicity, migrant or seasonal farmworker status, and home language, among other factors. Some school districts in New Jersey are likewise required to conduct community needs assessments. In other states, regional governing bodies determine the characteristics and needs of children in their service area. For example, North Carolina depends on local pre-kindergarten advisory committees that identify children in the community who would qualify for pre-kindergarten and work with the community to identify ties to those groups. Data must be disaggregated to prevent upholding stereotypes and overlooking some groups. For example, over 17.5 million members of nearly 50 different races and ethnicities are categorized as monolithic Asian American and Pacific Islanders and hailed as the “model minority.” As a result, communities such as Hmong Americans, who are less likely than the average resident to have a household income over $50,000, be employed, or be a college graduate, are at substantial risk of being underserved by local, state, and federal governments. Additionally, Hmong Americans, unlike some other Asian Americans, endured war, refugee camps, and harrowing migration, and thus, experience many traumas.
Simplify Enrollment
Programs serving diverse populations have worked in various ways to streamline and facilitate the enrollment process for families. This can involve simplified application forms, enrollment assistance, and flexible times and locations for enrollment. Some programs design processes to facilitate immigrant inclusion, such as not asking for parents’ or children’s Social Security numbers; translating forms, related web sites, and informational materials into common languages spoken by immigrant parents; allowing flexibility in the types of proof of residence and other documentations; and not requiring proof of income unless necessary.
Programs can offer to help families with health screenings and immunizations requirements by connecting families to partners who provide low-cost or free healthcare to young children. This helps immigrant families who struggle to afford the cost of taking children to the doctor since immigrant families are more likely to lack health insurance than U.S. families overall. Programs can offer a centralized registration to include interpreters, health providers who can complete required health screenings, and representatives from social service agencies who can respond to any broader family issues that might arise in the enrollment process.
Outreach, Staff Recruitment, and Training Activities
A recent analysis of infant and toddler early learning guidelines in 21 states found a lack of attention to the developmental and learning needs of dual language learners. States can pay for ongoing training that is intended to help providers and teachers work towards improved cultural competency. States can also work with childcare resource and referral agencies to create professional development plans that incorporate culturally and linguistically appropriate training and partner with community-based organizations with expertise in providing training services to English learning childcare providers. Additionally, states can offer scholarships and grants for diverse providers to attain education and training or increase compensation for bilingual childcare providers to retain a diverse early childhood workforce.
Teachers and staff at all levels of diverse racial, ethnic, and linguistic backgrounds need to be recruited and supported to work with diverse babies and toddlers. States can require programs to report on their plans for outreach in the underserved communities, on how they get the word out about the program to at-risk populations, on development and implementation of a coordinated process for recruiting, identifying, and enrolling at-risk young children, and on written plan for working with children and bilingual families. In light of the rapidly changing immigration policy contexts at local and national levels, offering cultural sensitivity training can promote trust from families from all national origins.
Parents can be reached directly through information packets for new parents in multiple languages that discuss quality childcare, availability of childcare assistance, and other benefits and services for their children. Several states offer kits to parents of all newborns in the state before they leave the hospital or birthing center, with information and resources to help parents care for their child, including tips about child development, health and safety, quality childcare, and school readiness only in English, positioning immigrants as a marginalized community. First 5 California, as an alternative example, offers kits available in English, Spanish, Chinese, Korean, and Vietnamese. These kits can also be distributed through clinics, doctor’s offices, community centers, and libraries.
Word of mouth from family, friends, and community organizations remain the primary source of information about early education and care services. States can provide funds to community-based organizations and immigrant-serving nonprofits to develop general information about childcare programs in appropriate formats and in the primary languages of immigrants in their communities. In some cases, policymakers have sought to place early education programs in targeted community-based organizations to reach immigrant groups that are under-enrolled in prekindergarten. Georgia, for example, is currently working to place pre-kindergarten programs within community-based organizations. The Wisconsin Department of Workforce Development, as another example, contracts directly with a migrant services provider, United Migrant Opportunity for bilingual childcare services that meet the needs of migrant and seasonal farmworkers.
In order to introduce early education and care to immigrant families, who are unfamiliar with non-parental care for young children, care systems need to work closely with refugee resettlement centers and community and religious leaders. Meet immigrant families where they already go, such as festivals and gatherings and at apartment complexes with large immigrant populations. Programs can pass out information or post flyers at popular locations, such as groceries stores, laundromats, doctor’s offices, faith-based organizations, refugee resettlement offices, libraries, English as a Second Language classes, adult education, and citizenship classes. Programs should work with staff at those agencies to explain available prekindergarten programs and how parents can find out more information and apply. Because WIC is available to children up to age five, regardless of parents’ immigration status, it is a particularly good location for reaching pre-kindergarten-eligible children of immigrants. Newark Public Schools has used more intensive in-person outreach through door-knocking campaigns, organizing community leaders to lead teams in door-to-door outreach to promote prekindergarten programs.
States that have done a great job at enrolling children of immigrant families have explicit state requirements to do so:
- Florida has a constitutional amendment requiring pre-kindergarten access for all four-year-olds and now has an 80 percent enrollment rate.
- Maryland has a state law that low-income children who qualify for free or reduced price lunch must be guaranteed a seat in a pre-kindergarten program from the day they show up to enroll, without a waiting list.
- New Jersey has 30 low-income school districts that are required to establish public, free pre-kindergarten programs, and must reach a target of enrolling 90 percent of four-year-olds in the district in pre-kindergarten. Because children of immigrants make up an overwhelming share of the overall population of children in these districts, programs in these communities apply substantial effort into mass media and in-person outreach in English and Spanish to reach all families in the area.
Trauma-informed Care
The ability for early education programs to reach large numbers of young children makes it uniquely apt as a critical context in which trauma-informed care can be delivered. However, the lack of training, resources, and racial bias has led to three- and four-year-old children being expelled at significant rates—over three times—than those in kindergarten through 12th grade. As a result, mental health issues that lead to challenging behaviors remain unaddressed. Young children are removed from all the benefits associated with early education, placing even more burden on parents to deal with a problem that is largely systematic as a personal failing. Moreover, Black children attending state-funded pre-kindergarten are twice as likely to be expelled than white children. Because one-in-10 Black people in the United States are immigrants, it is imperative to note that there is no such thing as a “Black issue” versus “immigrant issue.” Racial bias can be amplified with young children of immigrants whose culture and native language may be foreign to early education teachers and staff. Moreover, few practitioners have the skills needed to recognize and implement trauma-informed interventions within early childhood settings.
The high expulsion rate also indicates that parents and caregivers need help, starting from birth, to support the social and emotional development foundational for learning, future relationships, and school readiness. Work conditions, including low salaries, long hours, and high teacher-to-child ratios, may contribute to teachers feeling stressed or depressed, affecting their behavior management skills or tolerance for potential symptoms of trauma. As a result, supporting staff wellness is critical to any trauma-informed approach in early education programs. Staff needs access to early childhood mental health consultation to assist teachers, enforcement of lower student-teacher ratios, reasonable hours, and support to address secondary stress and related turnover.
Nationwide, early childhood programs are being encouraged to implement policies to reduce and eliminate preschool expulsion. The recently revised Head Start Program Performance Standards clearly prohibit expulsion due to children's behavior. Additionally, policymakers and providers are more knowledgeable about trauma-informed practice, which recognizes that children's history of trauma impacts their development, learning, emotions, and behavior.
Government funding and initiatives are needed to promote coordination of services that provide comprehensive training for staff, create safe and supportive early learning environments, and address cultural and linguistic needs. Adopting a trauma-informed philosophy requires a paradigm shift that begins with understanding that challenging behaviors are normal reactions to trauma and not intentional misbehavior. Programs such as Early Head Start and Head Start with access to infant/early childhood mental health consultation report less expulsion. In addition to general trauma-informed training, early education programs need to invest in language access, cultural-sensitive training, and understanding of challenges particular to young children of immigrants. Wraparound services are necessary to strengthen families, promote relationships, decrease parental stress, and improve family safety and financial security.
Nationwide, early childhood programs are being encouraged to implement policies to reduce and eliminate preschool expulsion. The recently revised Head Start Program Performance Standards clearly prohibit expulsion due to children's behavior. Additionally, policymakers and providers are more knowledgeable about trauma-informed practice, which recognizes that children's history of trauma impacts their development, learning, emotions, and behavior.
Build Positive Relationships with Parents
Another, less named, resistance towards early education is the concern that young children would forget their families’ cultures and languages. Malaly Hermat, 44, an Afghan refugee who now has U.S. citizenship, does not want her four-year-old daughter Sansa to attend preschool regardless of its potential benefits. Hermat married when she was 13-years-old and raised six children without preschool in Afghanistan. She has been following her own customs of raising her children and takes pride in her way of life. Hermat’s story reminds community organizers and policymakers that refugees do not flee without looking back to their home. Sansa is an outgoing and bossy child, whose confidence is no doubt a result of the doting attention of her mother.
Families (including chosen families) are young children’s first and most important teachers. Developmentally appropriate practices for young children should be informed by knowledge of young children’s social and cultural contexts, according to the National Association for the Education of Young Children. Strong partnerships between parents and providers enhance children’s social, emotional, and cognitive development. In Sansa’s circumstance, valuing the home culture and language might be the only way to draw her to preschool.
Engaging parents through reciprocity, trust, honesty, respect, and sensitivity is also the basis of a trauma-informed culturally responsive relationship with families. Honor diverse family structures and recognize and strive to counter the historical bias toward idealizing (and conversely blaming) biological mothers as primary caregivers. Early education programs can help families nurture their child’s social and emotional development by connecting them with pediatricians, parenting groups, and home visiting services.
Because parents and caregivers may also be trauma survivors and express their own fight, flight, and freeze survival responses in their interactions with teachers, teachers must respond to resistance or lack of engagement from parents with empathy, patience, and a lack of judgment. Teachers need to be prepared that it may take additional time to build trust with parents as their own histories may lead them to struggle to build trust in relationships with other adults. Families are best supported in facilitating their children’s development and mental health when services are available in their native languages.
Orientations, home visits, and open houses can build ties between schools and immigrant parents to the extent that parents feel comfortable participating and have positive interactions during these occasions. Schools offer parents leadership and advisory roles. Parent-led outreach is particularly effective, since they can communicate to one another in their home language and in a culturally appropriate manner. The Community Action Project in Tulsa, Oklahoma, for example, has a “captain” program that provides gift packs to parents who successfully recruit other families for the Head Start program. Portland Public Schools in Maine hires immigrant parents to serve as outreach workers. In Chicago, several agencies and organizations have collaborated to create a Head Start Ambassador program, in which parents are trained to reach out to Head Start-eligible families and encourage them to enroll.
Establishing relationships with parents can also create a sustainable early education workforce, in which eight in 10 providers cite a staffing problem, and half of providers stated hiring as harder than before the pandemic. Childcare centers also struggle with retention with a roughly 30 percent turnover rate each year. And yet, Parents In Community Action, Inc. (PICA), the federally designated grantee that operates Head Start programs, has staff members who have been there for decades. Over 70 percent of its staff are parents whose children are in the program or have graduated from the program. Following a two-generation approach, PICA offers a number of training programs to help parents learn new skills, gain hands-on work experience, and prepare for the future.
Family, Friend, and Neighbor Care
Family, friend, and neighbor (FFN) care is the oldest and most common form of childcare among all families. Families may choose FFN care because it is the option that is most comfortable and familiar, most flexible, most affordable, or provides children with the most individualized attention. In 2016, 60 percent (12.8 million) of the 21.4 million children under age six were in some type of regular childcare arrangement in a typical week. Since early 2020, due to the COVID-19 pandemic, FFN care became the only option for many families. Families, hesitant to enroll their children in large group settings, increasingly sought out FFN care during the pandemic. By early September, the percentage of households using FFN and other home-based care exceeded pre-pandemic levels. Although FFN providers outnumber center-based providers and serve more children, FFN care is largely undervalued by federal and state policymakers.
Justine’s preference for her children to be cared for by her aunt reflects the prevalent use of FFN care among immigrant populations. In addition to lower cost and flexibility in location and service-hours, these caregivers often share language and culture with families of the children in their care, and thus, offer a trusted, safe, and high-quality experience that is responsive to the families’ priorities. These providers can offer cultural continuity that can strengthen cultural identity and child-parent relationship. Parents and providers can work together on curriculum and values whereas language barriers make it difficult for parents to connect with more formal childcare programs.
Many immigrant parents believe that FFN care provides more personal attention for their children. Indeed, research shows that FNN providers often have low adult-child ratios, suggesting that these providers are able to spend more individual, quality time with each child. Although studies show that overall, the quality of FFN care is suboptimal to licensed programs, researchers are wrestling with appropriate assessment tools for FFN providers. The studies that show that center-based care predicts higher levels of cognition for children ages zero to three in the United States does not necessarily demonstrate that informal care cannot produce the same results. The potential of FFN care has yet to be measured due to its invisibility, diverse forms, and lack of financial and institutional support.
What is certain is that many families, especially immigrants, will continue to prefer FFN care and the early education and care workforce requires FFN providers to fulfill the demand for childcare. Increasing legislative and financial investments in FFN caregivers promote equity for immigrant families; it supports these workers, enhances the quality of care, and lessens the overburdened care industry. Offering immigrant parents and their informal childcare providers additional resources, including training, technical assistance, and access to subsidies, is critical in order to enhance access and improve child development outcomes.
Half of all immigrant caregivers in the early education workforce are providing private home or family-based care. A quarter of family-based providers in the United States identify as Latinx. Because childcare programs and resources are generally focused primarily or solely on licensed providers and are often limited or unavailable for FFN (license-exempt) providers, the majority of FFN providers earn on average merely $7,420 a year because parents and guardians are the only sources of payment. Even prior to the pandemic, nearly 22 percent of immigrant ECEC providers were living in poverty. This lack of appreciation or fair compensation is part of a broader, historical trend wherein work done by women of color within private homes is not recognized as “real” work either by the public or policymakers.
The Child Care and Development Block Grant biennial state plans found that only three states report that they have policies in place to make their childcare licensing regulations more accessible to providers from language minority or immigrant communities. Moreover, many immigrant FFN providers are not culturally connected and know that these subsidies are available. Spanish-speaking FFN care workers were half as likely to access subsidies as their English-speaking peers. Some states, including Florida and North Carolina, prohibit unauthorized immigrants from collecting any subsidies. Unsurprisingly, only 38 percent indicated that they received subsidies or other financial support other than payments from parents, compared to 74 percent of English-speaking FFN providers. Most states allow unlicensed childcare providers to receive subsidy payments, but a report in January from Home Grown found that the accessibility and amount of funding unlicensed providers get varies. Most states require household-wide background checks to receive payments, which experts say can make it less likely that undocumented providers or providers in mixed-status households will apply for assistance.
Immigrant providers, specifically, are often discouraged from becoming licensed due to costs, language barriers, and real or perceived barriers related to their immigration status. Expensive and onerous requirements dissuade care providers from applying for a childcare license. There needs to be a concerted effort to reduce legislative and administrative barriers to support immigrant FFN care providers. This can look like simplifying application processes, translation in multiple languages, revision of documentation requirements, and community outreach—the same mentioned recommendations for all public programs to reach immigrant families.
Yet another solution is creating funding avenues for FFN providers without requiring license. The Child Tax Credit provides flexibility for parents to use money how they want, trusting parents to find the best care for their children based on their specific needs, which might include linguistic and cultural continuity. Disability and elderly care can provide a sustainable model of family members receiving government payments to do care work.
Training and funding for FFN providers chosen and trusted by immigrant parents can be a way to promote culturally inclusive early education and care for their children. Some states have initiated training for refugee parents to become childcare providers, promoting additional income for refugee families and culturally competent environments. States can support providers who care for children who are linguistically diverse by offering financial incentives. California, for example, pays providers who care for dual language children at an adjusted childcare subsidy payment rate that is 10 percent higher than the state standard reimbursement for contracted providers.
States need to provide dedicated funding directly to providers and community-based organizations that work with FFN and immigrant providers. For example, in 2021, Minnesota Department of Human Services directed $1 million of the $48 million in federal CARES Act funding to state and local agencies working with FFN providers. $800,000 of the million went to four existing department grantees serving FFN providers across the state, with a focus on the Somali, Latinx, American Indian, and immigrant communities. The remaining money was distributed to small agencies, which must be at least 51 percent owned by a woman, racial minority, or person with a substantial physical disability.
FFN support programs can collaborate with trusted community organizations to personalize outreach at strategic locations, word of mouth, and going door-to-door. Training for immigrant FFN care supporters should be trauma-informed. Immigrant FFN providers carry many stressors: family-related stress, financial burdens, immigration-related stress, burnout, primary and secondary trauma, limited developmental knowledge and child rearing strategies, depression, anxiety, and social isolation. The caregivers’ wellbeing is inextricably and intimately connected to the mental health of the young child, impacting the children’s long-term achievement. The Pamoja Early Childhood Education Workforce Program in Colorado, for example, offers immigrant mothers a trauma-resilient training in several languages to do home visits with people who are already or interested in becoming FFN providers. With a grant from the Colorado Health Foundation, the co-organizer Lauren Dorn names FFN care as a “form of healthcare, … where the children are getting their brain growth, all of their positive, emotional, shared connections.” This program intervenes in the caregivers’ trauma and positions immigrant women in the role of teaching each other. In addition to advancing kin care, Pamoja offers a community to immigrant women, who are often isolated in their homes.
Innovative partnerships with Head Start and university groups allow immigrant families to tap into established and funded resources that can readily be tailored to respond to their specific needs. Another way to help support immigrant providers is to develop community networks for FFN providers through gatherings at local parks or community centers to share information and ideas. All Our Kin, a nonprofit group advocating for family childcare providers in Connecticut and New York, helps Spanish-speaking FFNs navigate the licensing process and helps FFN providers who aren’t looking for licenses to get access to other resources. Additionally, give immigrants a seat at the table to seek input from them in developing childcare policies and programs.
Whole Family Solutions
Enhancing the wellness and success of children of immigrants requires two-generation (or whole-family) strategies that recognize the intersection of several systems: early education and care, adult education, immigration policies, and health and social services. As explained, trauma results from structural and political circumstances that impacts the entire family. Social service staff, early education educators and caregivers, and home visiting case workers need trauma-informed training to recognize early signs of trauma and appropriately intervene across cultures to help young children and their families, which will yield life-long benefits. Since all refugees pass through resettlement programs, these agencies can improve and standardize mental health screening processes for adults and their young children and guide them to the relevant services.
All solutions need meaningful community outreach and make a real commitment to language access that includes investments in translation of informational materials and bilingual staff and interpreters. Because the stresses, work conditions, and overall wellbeing of caregivers profoundly impact young children's cognitive and emotional development, comprehensive support services for families will promote the best growing conditions for young children. The report highlights five additional ways to help immigrant families:
- Home Visiting Programs: Although they underserve immigrant families, like other social programs, home visiting services can particularly provide long-term and far-reaching impact, acting as a stepping stone for critical programs, such as counseling, early education, and job training.
- Pathway to citizenship: A pathway towards permanent residency and citizenship reduces the chronic stress on the entire family, which have been shown to harm children’s social and cognitive development.
- Social Services: All public services are futile if they cannot reach the most vulnerable population, and therefore, need to be accessible to children of immigrants.
- Work Authorization: Work authorization and labor protection prevent exploitations of undocumented and documented immigrants, allowing them to earn more wages and more time with their children.
- Upskilling Opportunities: Immigrants can fill many underemployed positions, mutually benefiting the U.S. economy, meet people’s needs, and help immigrant families if upskilling opportunities are financially and linguistically accessible.
Home Visiting Programs
Home visitings, family-focused social service programs that visit expectant mothers and caretakers alongside their young children at home, are a uniquely promising intervention for reaching children of immigrants through a whole-family approach. Home visitings have been shown to benefit the whole family, strengthening children’s linguistic and cognitive development and their school readiness, increasing parents income, employment rates, and school enrollment. In addition to the Maternal, Infant, and Early Childhood Home Visiting Program, a federal home visiting funding initiative, states and counties have expanded investments in local family visiting programs.
Despite its shown benefits, home visiting services–like other public programs–have underserved dual language learners and children in immigrant families. These families may face barriers to participating in home visiting programs due to language barriers, lack of culturally and linguistically trained program staff, and hesitation to access social services (e.g., early childhood education, health, nutrition) due to fear of immigration consequences.
Home visiting programs can partner with local-based organizations already serving these immigrant families to recruit, engage, and retain these families by informing them about the existence, eligibility, and benefits of home visiting programs. Home visitings—if they adapt cultural and language strategies to reach immigrant families—would likely see tremendous results with immigrant families since they are disproportionately likely to face risk factors, such as poverty and low parental education. Home-visiting can build trust and remove several access barriers, such as transportation and reduce anxiety of encountering federal agents. Staff can better see the family’s needs since members are more comfortable at home and target their specific needs through providing information, training, screenings, and connections and referrals to services for parents expecting or caring for young children.
Because these visits happen in individual families, they can be an opportunity to address trauma in a way that does not feel foreign or stigmatizing for immigrant families. For example, RefugeeOne Wellness Program, a mental health program in Illinois, integrates a home visiting program for trauma-exposed pregnant mothers and families with children under age 3 of refugee/immigrant status. The program sends a team of clinicians, psychiatrists, and interpreters in immigrant homes, regarding the parent as an expert through a partnership to support both child and parent goals. In addition to strengthening the parent-child relationship and promoting child development, staff can introduce immigrants to programs and guide them in cultural navigation that have been restrictive for immigrants.
Pathway to Citizenship
Many children of undocumented parents have poorly developed cognitive skills, visible in children as young as twenty-four months, because their parents avoid accessing valuable resources, live isolated from social networks, and work in exploitative conditions. Hirokazu Yoshikawa presents quantitative data to show that having an undocumented parent harm children’s development, especially their early cognitive skills. The parent’s citizenship status does not inherently impact the child’s well-being—the policies tied to citizenship status do.
An opportunity towards citizenship advances children’s cognitive skills, development, and overall health. A path to citizenship and end of public charge rule would increase the use of public programs and childcare subsidies and enrollment in programs to improve parents' job skills and education, such as GED classes or job training. Immigrants need clear and honest announcements whether those who receive parole status can access social services, many of which are essential to give children’s food security, health insurance, and early education and childcare. States can intervene to help immigrant families acquire necessary resources. Colorado, as an example, has passed a law that eliminates lawful presence in the United States as a possible factor in determinations of eligibility for any state or local public benefits in 2021.
Social Services
Social services must center immigrants rather than treat the immigrant population as a niche population. The enactment of the Personal Responsibility and Work Opportunity Reconciliation Act in 1996 reflects a shift in U.S. social policy to increasingly stratified immigrants—not only to undocumented immigrants but also to lawful permanent residents and U.S. citizens in immigrant families. As a result, children in immigrant families have not been able to fully realize the benefits from social safety-net programs—including the 2020 Coronavirus Aid, Relief, and Economic Security Act stimulus payments.
The COVID-19 pandemic, which presented a unique opportunity to lessen the harmful effects of stratification by legal status, provided a model and opportunity to reexamine immigrant exclusions, restrictions, and administrative burdens in public programs. Under the American Rescue Plan Act, an estimated 27 million children became newly eligible for the fully refundable portion of the child tax credit; this recognition should be made permanent. A more inclusive social policy needs to modify eligibility to depend on the health and developmental needs of the child, especially regarding nutrition and medical services, not the immigration status of the household. The utility of public charge has consistently harmed immigrant parents and children, and thus, must be removed in order to restore trust in health services and other life-saving programs for our children.
Additionally, social programs require real language accessibility, including translations in multiple languages, multilingual staff, and collaboration with community organizations. School district–based providers reported drawing on federal funding streams for outreach activities. For example, Title I grants can be used on immigrant outreach and parent engagement. Grants from Title III funds, allocated for education agencies for serving students with limited English proficiency, can support immigrant/refugee services.
Work Authorization
As the Build Back Better Act appears to be permanently halted since its passage in the House, it’s worth noting how close legislators were to helping immigrant families in three main ways: long-term work permits for immigrants to support their families, health care coverage expansion to immigrants and their children, and necessary funding and priority to fix the childcare crisis.
The immigration provisions in Build Back Better offer up to 10 years of work authorization for undocumented people living in the United States. The parole provisions provide temporary status. It also allows visa recapture, preserving some 222,000 unused family-based visas and roughly 157,000 employment-based visas that would otherwise lapse. The labor shortage provides an opportunity for the state to partner with employers to offer training for immigrants.
Work authorization must go hand-in-hand with labor protection for all immigrants. Many undocumented immigrants do not have work protection, such as the right to be paid at least the minimum wage, the right to be paid for overtime hours, the right to take meal breaks, access to workers’ compensation when injured, and the right to advocate for better working condition. Unionization provides a structure within which undocumented workers could be assured basic legal work conditions through a collective bargaining. Contrary to assumptions that immigrants are unorganizable, evidence supports the reverse: immigrants tend to be more inclined towards unions than the native born. The success of the Justice for Janitors campaign of the Service Employees International Union and the mobilization of drywall hangers in residential construction indicates the importance of engaging Latinx immigrants.
Education and Workforce Development
The Build Back Better Act would have increased the maximum award amount for Pell Grants, subsidies created in 1965 for undergraduates of low-income families, who are actively attending universities and or other secondary institution, which are critical for first generation students, low-income students, and students of color to help build their futures, and would have ensured DREAMers—young undocumented immigrants who would’ve benefited from the Development, Relief, and Education for Alien Minors Act—could access Pell Grants. Over half a million children in the United States have a parent who is a Temporary Protected Status or Deferred Action for Childhood Arrivals recipient. Allowing DREAMers to access Pell Grants place the whole family on a more promising path to earn more money, job satisfaction, and overall health. The creation and scaling up of opportunities for parents to develop knowledge, skills, and social capital can lift their families’ intergenerational trajectories because the social and material resources that higher level of education confers are passed down across generations.
While offering Pell Grants to DREAMers will make a significant impact, professionalization opportunities should be offered at all levels. After Washington, D.C. passed regulations that sought to increase the education and credentials of the early educator workforce in 2016, the University of the District of Columbia Community College designed and implemented a Spanish-English bilingual associate degree program. This program aimed to address academic, bureaucratic, linguistic, and other barriers to obtaining degrees by providing early childhood educators with the opportunity to take courses in Spanish at close to no cost to participants. Pamoja Early Childhood Education Workforce Program offers free college-accredited courses in four languages, Swahili, Arabic, Farsi, and Karen, and connects them with mentors to help with homework and technology skills—all of which ensures each woman completes her certificate and become a lead teacher. To reduce financial burdens, Pamoja also offers compensation for missed work time to attend class and provides payment to friends or family members who care for their children during class or practicum time.
Briya Public Charter School in Washington D.C., as another example, provides a whole-family approach through free high-quality early education to children and tuition-free high school diploma, Medical Assistant Program, and Child Development Associate Program to immigrant parents. The Child Development Associate Program is taught in English and Spanish, opening opportunities for more multilingual child educators. Founded in 1975 in response to the influx of refugees after the Vietnam War, Briya has touched tens of thousands of families. As the parents learn and grow their own skills, their young children enroll in the early education and care program at the same location. Additionally, three of the four locations also offer health services through the Mary’s Center, a community health center. Recognizing the trauma experienced by many immigrants and refugees, Briya uniquely provides mental health and behavioral health counselors within their schools. Counseling can be a foreign concept to Briya’s students, so participants might begin by staying after lunch or classes to talk about safe parenting before they start individual counseling sessions.
Corrected at 7:15 am on May 20, 2022: This report has been changed to correct the description of Pamoja Early Childhood Education Workforce Program. The program does not pay students in the workforce program to enroll. It does provide compensation for missed work time to attend class and provide payment to friends or family who care for their children during class or practicum time. Pamoja does pay participants in its home visiting program, in which candidates are trained to do home visits and to go into their communities to teach in the home with parents and caregivers.
Conclusion: The Potential to Thrive
The growing population of young children of immigrants have tremendous potential to thrive, be happy, and contribute to the U.S. society and economy. The challenges they face result from geopolitical and structural circumstances, and therefore, can be mitigated through systematic investments.The suggested strategies are well-researched and have already been applied in different communities. Their future will be matched by the ways the United States lives up to its promise of the "American Dream."
Soor Gul Entizar, who worked for the U.S. government at the Department of State Annex in Afghanistan, recently resettled in Arizona with his wife and five children after the August evacuation of U.S. troops from his country of origin. They already have an U.S.-citizen in their family, a month-old Arizonan native. He dreams that his children can complete their education. With animated, laughing eyes, he adds that he’d love for them to be engineers or maybe Obama! He jokes because the future is still far from his mind.

As of right now, it is very unlikely that Soor Gul’s children will ever attend any form of preschool. Like the other refugees in this report, he and his wife, Sarqas, do not know the available education options before first-grade. Although virtually all refugee parents with children up to age five will meet the income-based eligibility requirements for Head Start services, these families do not know about Head Start and refugee resettlement agencies are not responsible for helping refugees enroll their young children in programs.
Even Soor Gul’s oldest children, seven-year-old twins Naila and Nabila are not enrolled in school, despite having been in Tucson for months. Connie Phillips, CEO and president of the Lutheran Social Services of the Southwest, states that school enrollment simply has not been a priority, given the lack of resources and capacity the organization faces. While the Lutheran Social Services of the Southwest has been resettling refugees since 1975, the Trump administration immigration policy, COVID-19 pandemic, and housing crisis have completely changed the conditions of resettlement. The Trump administration devastated the resettlement system: the number of refugees admitted to the United States dropped by 86 percent from 2016 to 2020. Because of the sharp decline of arrivals, the agency decreased its staff, lost relationships with partners and local organizations, and dealt with budget cuts: “we just didn’t really have … our processes in place.” On top of this, the nationwide housing crisis requires many arriving refugees to stay temporarily in hotels or Airbnb, often moving more than once. Case workers delay enrolling children in school until they’re in permanent housing without a clear idea of when permanent housing will become available.
As a result, refugee children are isolated with their families rather than making new friends or learning English and other school subjects. Moreover, these children must negotiate their trauma and their parents' trauma alone. The violent deaths of family members are not an exception, but a common fact for many Afghan refugees, who will soon be, if they aren’t already, a significant part of communities across the United States. Soor Gul presented a picture of his brother, murdered one month after Soor Gul boarded a U.S. plane. His brother was targeted because of Soor Gul's escape to the United States. He showed a photograph of another brother, whose face is deformed by a Taliban member’s bullet. Next, a picture of two brothers in military clothes, who have also been killed by the Taliban. He says nothing about guilt or grief—just a visual catalog of his losses. Soor Gul explained that he never imagined that the United States could lose the war. He only learned of the imminent threat to his family’s lives when his U.S. superior commanded him to hand over the weapons to the Taliban. He was stupefied.
In addition to the many deaths of family members in Afghanistan, other Afghan families detailed family separation. Zahra Mohammed, whose husband stayed behind in order to take care of his parents, is now a single mother to her three-year-old daughter. Aziza Salehi, whose husband was too sick to escape with her, shared the grueling details of being at the overcrowded Kabul airport with eight children: one of her daughters fainted because they did not have any food for the three days they spent at the airport and a son unable to walk because his feet bled heavily after he lost his shoes in the dense crowd. A sympathetic man wrapped her son’s feet with papers and carried him for the rest of their time at the airport. Aziza has chronic back pain due to the arduous journey. Aziza counts every single day that has passed that she has been away from her husband. Still she expresses feeling both relief and good fortune—many people, especially elders and children, died in the airport. None of her five children under the age of 18 has been enrolled in school by a caseworker. The eldest three brothers, 18-, 19-, and 20-years-old, will all work to take care of the family.

As the paper has discussed, the number of children in the United States who will have been subjected to such difficult conditions and whose parents are unable to provide them all they need to cope with it is growing. Failure to intervene in the children’s trauma and stress can harm their cognitive and socioemotional development. Along with Azizi’s and Soor Gul’s children, Joseph, Kingston, and Queen Elizabeth all deserve an equal chance to complete their education, which begins with the foundation of early learning and care. The very possibility of children of immigrants to attend college to become an engineer or public official is a very serious promise that the United States has made to children since its inception. The failure to uphold this promise undermines our democracy that depends on every voter to maintain its legitimacy. Whether children of immigrants—a population that is expected to be one-third of the U.S. child population by 2025—experience healthy development will profoundly affect their roles as future citizens, workers, and parents. Our investments signal our values and priorities, and our investments in the children of immigrants now will determine the stability of the U.S. culture, society, and economy for decades to come.
More About the Authors




