
Designing a Local Mixed Delivery Model
For state-funded preschool programs, most states set basic policies or guardrails for mixed delivery, then largely leave it up to localities to decide how to implement their model. Similar design questions face localities looking to set up their own locally funded programs. There are a few big design choices that systems need to make first: Who is allowed to provide services, and how are providers selected to offer services? What does it mean to be a participating provider, contractually and financially? What role do school districts play?
By understanding how different places have approached these big decisions, system leaders can identify different potential roadmaps to follow in their own design work.
Who Is Allowed to Provide Services?
System leaders need to define which types of organizations are allowed to provide services. This is a critical foundational question—whether certain provider types are able (or not) to receive public funds has meaningful ramifications for their own financial viability. Some system leaders will do a landscape analysis of current-state child care use in their community to help make this decision, both to understand child care supply and family preference. Others may have a strong values-based perspective on which providers should be included. Some may be influenced by state regulations, or the advocacy of powerful interest groups and local political leaders. Most mixed delivery models at least include school districts and private providers; others vary based on local context.
Mixed delivery models may include any of the following provider types:
- School district: School districts almost always have a role in local early childhood systems, either as the administrator and a service provider or just as a service provider. In some places, the school district may have essentially the right of first refusal as a provider of early education services; this may limit how much capacity is available for other providers. In some places, there may be a limit to how much of the total service provision can be within public schools. For example, New York State requires that school districts contract at least 10 percent of preschool services to private providers, though waivers are available. In West Virginia, school districts must contract at least 50 percent of preschool services.
- Charter schools: In some states and localities, charter schools are treated no differently than school districts when it comes to preschool service administration; some states offer charters that include pre-K as a grade. In other places, charter schools are treated more like a private provider and required to apply to provide early education services.
- Private providers: Private, center-based child care providers are the most common participants alongside public schools in mixed delivery models. In 44 of 60 state pre-K programs, private agencies can receive funds directly from the state or be subcontractors to the entity that receives funds from the state (like school districts). The broad category of private providers includes nonprofit and for-profit centers and providers who receive Head Start funds directly from the federal government. While Head Start providers must be nonprofits by statute, many states and localities have not historically discriminated in their mixed delivery models based on tax structure or profitability. With the growth of private equity’s stake in early education, some places are setting restrictions on ownership structure or imposing profit caps. Private providers may also include religiously affiliated providers; in many communities, religious providers have played a critical role in early education initiatives to meet access goals without much public controversy. For example, New York City partners with a range of religious providers in its universal preschool program. In other places, however, the question of what role religious providers can play has been a lightning rod. At the national level, the role of religious providers in a potential federal early childhood program was a big sticking point in conversations about Build Back Better. In Colorado’s state preschool program, this was settled through litigation.
- Home-based providers: Home-based child care providers are both popular and essential, but they are not always integrated into major early care and education programs. As public preschool programs have expanded, many have explicitly—or inadvertently—excluded home-based providers. Many system leaders are now taking intentional steps to more explicitly design their local early education initiatives to be inclusive of home-based providers, recognizing this will more fully meet family needs and support the broader early education ecosystem in their communities. (See our prior blog post on this topic, “More Options for Families: Public Preschool in Family Child Care Homes.”)
- Informal providers: Informal providers—also referred to as unlicensed, unlisted, or license-exempt, depending on the state—play a large role in local early education ecosystems. These providers serve smaller numbers of children and are less formally regulated, but often provide more flexible care options that meet family needs and preferences. Some states allow informal providers to participate in their child care subsidy system and to receive reimbursement for serving income-eligible families. It is far less common for informal providers to participate in other publicly funded early education initiatives, like state or local preschool programs.
Localities typically need to decide which providers are eligible to provide services in general, and to which age groups and which services specifically. For example, in New York City, home-based providers are able to provide preschool services to three-year-olds, but not four-year-olds; private providers play a large role in service provision overall, with fewer than half of all preschool students served by the school district. In Chicago, four-year-olds are primarily served in public schools and three-year-olds are primarily served in private child care programs. In Multnomah County, Oregon, the locally funded Preschool for All program prioritized small child care centers and home-based providers initially, ahead of larger centers and public schools.
Which Providers Are Eligible to Provide Services?
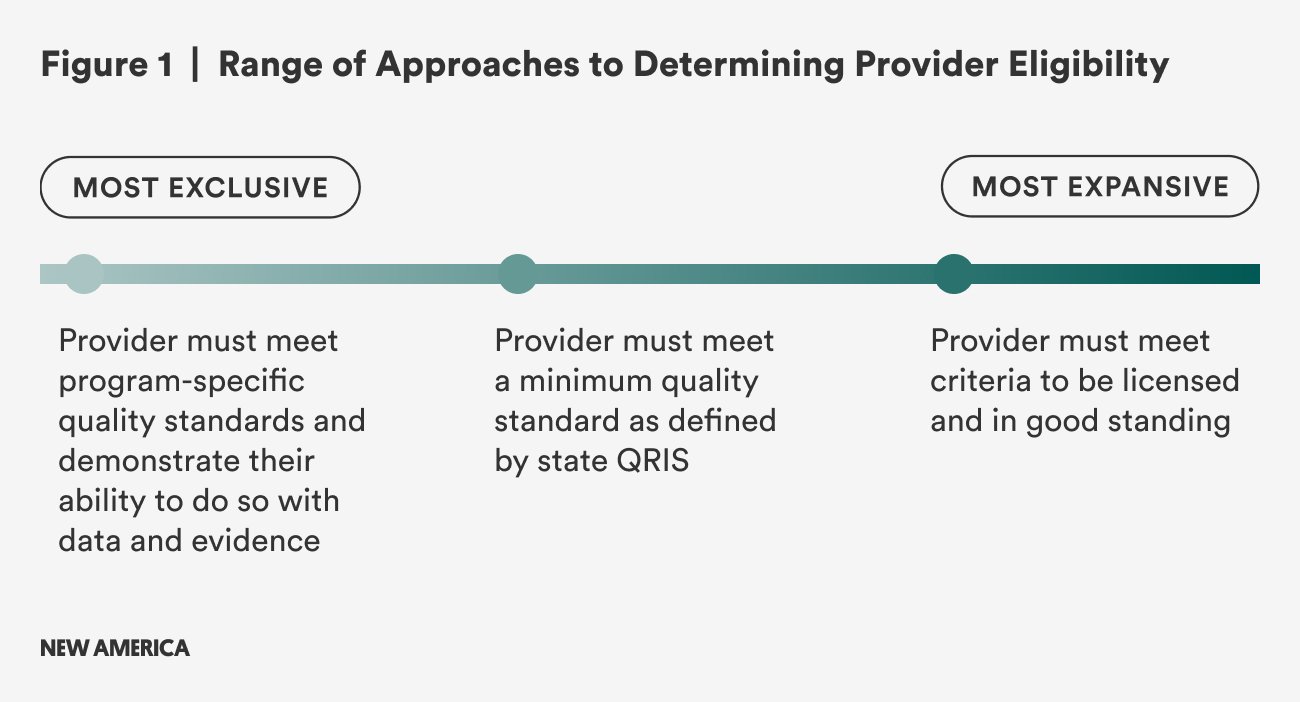
Once a system decides which providers can offer services, they must select who among the eligible providers will provide services. Systems vary in the threshold they define for what makes a provider eligible to provide services, as shown in Figure 1. Some systems simply require providers to be licensed and in good standing, which allows for the most expansive group of potential providers. On the other end of the spectrum, some systems define their own quality standards and require providers to demonstrate their ability to meet those standards with data and evidence.
Where systems situate themselves along this spectrum can be influenced by numerous factors:
- Is the baseline licensing standard strong enough that leaders feel confident in any provider who meets that standard?
- Are there other defined and accepted measures of program quality already in use in this community?
- Based on the quantity and quality of available child care provider supply, is there benefit to enabling a wider group of providers to serve as partners? Is there benefit to restricting access?
How Are Providers Selected to Provide Services?
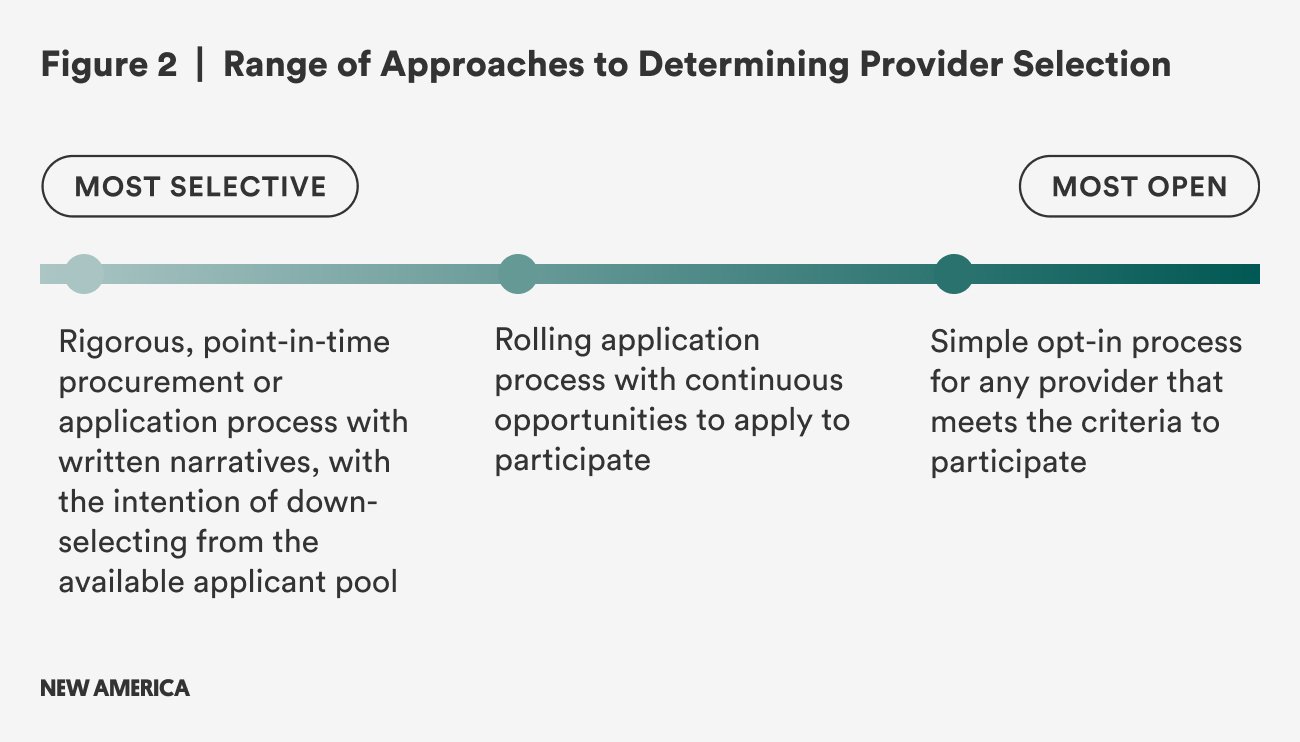
Once system leaders determine which providers are eligible, they must define a process to select which ones in particular will be able to participate. These processes range in how competitive or selective they might be (see Figure 2). A less competitive system may allow any provider that meets the minimum bar to opt in, while more competitive systems run a rigorous point-in-time procurement or application process with written narratives, with the intention of down-selecting from the available applicant pool. Some systems are held to strict requirements by their city or county procurement rules, which may require a more competitive process. Communities with abundant child care supply may use a competitive process to objectively identify the subset of providers needed to meet demand.
What Are the Impacts of Selection Design?
In designing the selection process and criteria for a local early childhood system, there are intersecting questions of capacity, quality, and equity:
- Will certain early education settings be advantaged over others? Who might be left behind by this process, and what impact will that have on services to families and children?
- How will criteria or processes for provider participation impact our capacity goals?
- How will this dynamic differ between neighborhoods? Do we risk creating a scenario where some neighborhoods have higher-quality providers than others?
- What beliefs do we hold about baseline quality required to offer services? What is our ability to support ongoing quality improvement?
- How can we create as much objectivity in the process as possible?
How localities address these design questions will have implications for the livelihood of early childhood educators and the experiences that families and children have. As with many topics in system design, there is not a single right answer, though lessons learned from the ECE Implementation Working Group can help leaders in other cities and counties understand the implications and unintended consequences of different decisions.
Equity for Providers
When the provider identification process is more exclusive and requires many process steps, providers may not be equipped to navigate the ins and outs of public procurement on their own. Well-resourced child care businesses may be able to hire grant writers, while less-resourced providers may not know about the grant or award process or how to apply. Smaller providers are inherently disadvantaged; this is particularly true for home-based providers, where the owner is also likely spending all of her time in the classroom.
More inclusive systems rarely land there by accident; their models are the result of intentional choices made well before launch. In Multnomah County, system leaders prioritized small providers when beginning expansion and explicitly designed processes around them. The provider application was designed to be extremely straightforward and offered in multiple languages, with an intermediary who could support providers rather than requiring them to contract directly with the county.
In New York City’s Pre-K for All program, providers were required to respond to a rigorous, competitive request for proposal to participate. This was in part driven by city procurement rules, but also by strongly held views about what quality should look like and how to measure it. Over time, New York City has evolved its procurement processes to consider multiple measures of quality and to make the process more inclusive.
Quality Considerations
In the early childhood field, there is robust research and evidence about how children learn and develop, how educators facilitate that growth, and how classroom environments support it. There are validated tools to measure various components of quality. However, this research is not uniformly integrated into the way that state and local agencies report on quality in early childhood settings.
How local systems define quality on an ongoing basis, including when selecting which providers can participate in a local initiative, may depend on what statewide systems are already in place. For example, Denver and Philadelphia reference their state Quality Rating and Improvement System (QRIS) when selecting providers for their locally funded preschool program. Multnomah County and New York City have defined their own quality thresholds. This choice can depend on local leaders’ perceptions of the state QRIS systems.
Based on many of the markers typically used in state quality rating systems, lower-income neighborhoods typically have a concentration of lower-quality early education providers. This is in part because many standardized quality measures conflate quality with resources: Providers with more certified (and higher paid) teachers typically score better on quality rating systems than those with uncertified teachers. Providers may receive additional points for state-of-the-art outdoor play spaces and other features of their facilities; those who are in older or shared spaces, like a church basement or a common space in a public housing development, may struggle to earn high marks for their facilities. While there are good reasons to set a benchmark for quality and stick to it, system leaders need to consider what this means for different parts of a community, who will be left behind, and whether the right variables are truly being measured.
For the purposes of including providers in a publicly funded initiative, system leaders are likely interested in both program and classroom quality (e.g., is this a positive learning environment for children?) and the quality of the business side of the organization (e.g., is the entity capable of meeting the administrative demands of participating in this public program). The minimum viable threshold for each of these measures will be different, and programs can be coached to build both competencies.
Support for quality improvement should be continuous, and explicitly funded, with ongoing coaching and professional development for providers when they enter the system and throughout their careers. Too often, quality improvement initiatives can amplify “in groups” and “out groups” or even create new ones, and administrators and providers are caught up in servicing a system that in reality does not work well for providers or for the families and children they serve. There are innovative approaches that meet the needs of the people who provide care, which in turn better support the families who are getting it. “Microcredentials” are a pathway to greater inclusion of providers in a quality-oriented system. In some places, there are multiple on-ramps for providers so that those who are not fully ready to provide services can be on a pathway where they work toward being eligible for publicly funded services. These types of programs can serve to raise the overall bar for early education provision in a community. When the Denver Preschool Program first launched, the share of providers in the city that met the quality threshold was low. However, with a $10 million investment in coaching over four years, Denver helped over 100 providers improve their quality to meet eligibility standards, thereby increasing the share of providers eligible to participate in the local program and driving up the caliber of early care and education citywide.
Some systems may face pressure to meet certain seat targets or access goals that push them to expand beyond the number of providers they assess to be of quality. There are long-term risks; in one ECE Implementation Working Group community, rapid expansion led system leaders to be more lenient about which providers were granted contracts. Several years into the program’s operations, some of those providers continue to have serious quality concerns, and administrators are facing tough political decisions about how to end their contracts.
Capacity Impacts
On the other hand, in some places the number of qualified, quality providers may outstrip projected need. If too many providers are invited into the system, there is a risk of oversaturating supply. In such cases, providers may not be able to fully enroll their programs. System leaders need to carefully map and consider how many slots are needed for each age group in each microgeography. Families tend to weigh distance as one of their top selection criteria for early childhood education and prefer not to travel long distances. In some places, this may mean mapping provider capacity within a zip code; in more densely populated places, smaller units of geography—such as census tracts or elementary school attendance zones—are more relevant. System leaders can look at past enrollment patterns, census data on birth rates, and other public administrative data sources to understand family demand, and then target the number of seats needed in a specific geography accordingly.
While it may feel exclusionary to keep some qualified providers out of the system, if there is too much excess capacity in the early childhood system, then providers will not be able to reach full enrollment and there will be a risk to their financial sustainability. Resource constraints may prevent administrators from inviting all providers to participate, particularly if the program is in an earlier phase of expansion and not yet serving all children in the city or county. In Philadelphia, the city’s preschool program does not yet have enough funding to fully meet demand citywide; however, there is a process for providers to be “prequalified” so that when more money becomes available, they can quickly be brought into the system.
Whatever the ultimate selection process is, it is important that administrators abide by local procurement guidance, carefully document the decision-making process, and remain consistent in approach. Inevitably, there will be disappointed providers, families, and elected officials, and administrators must be ready to defend and stand by their process, even in the face of potential lawsuits and political pressure.
What Are the Models for Provider Participation?
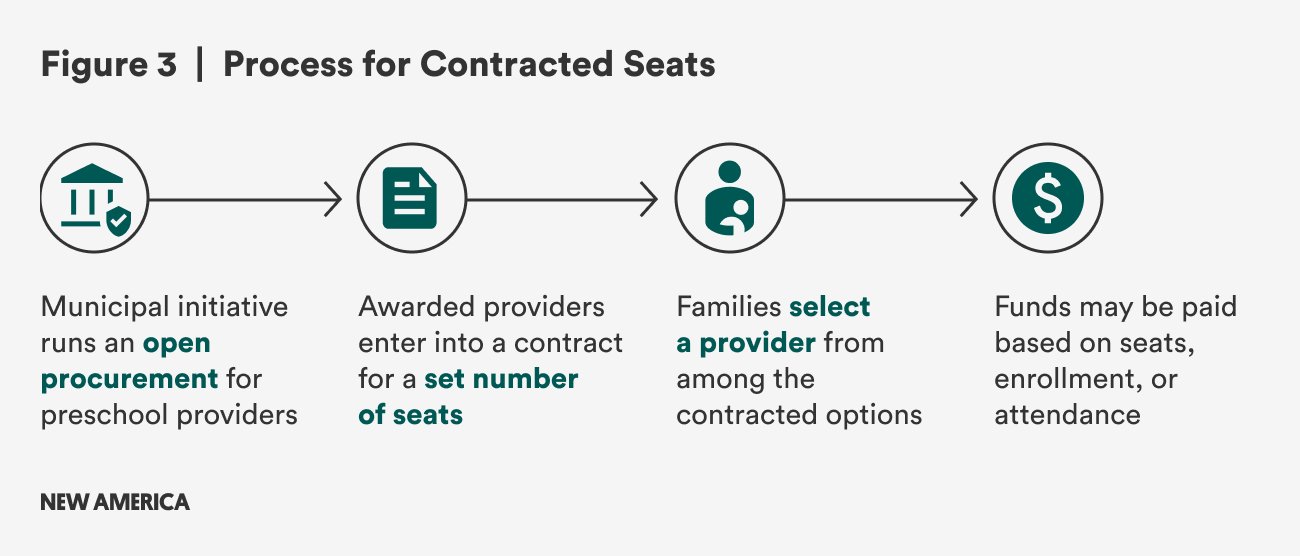
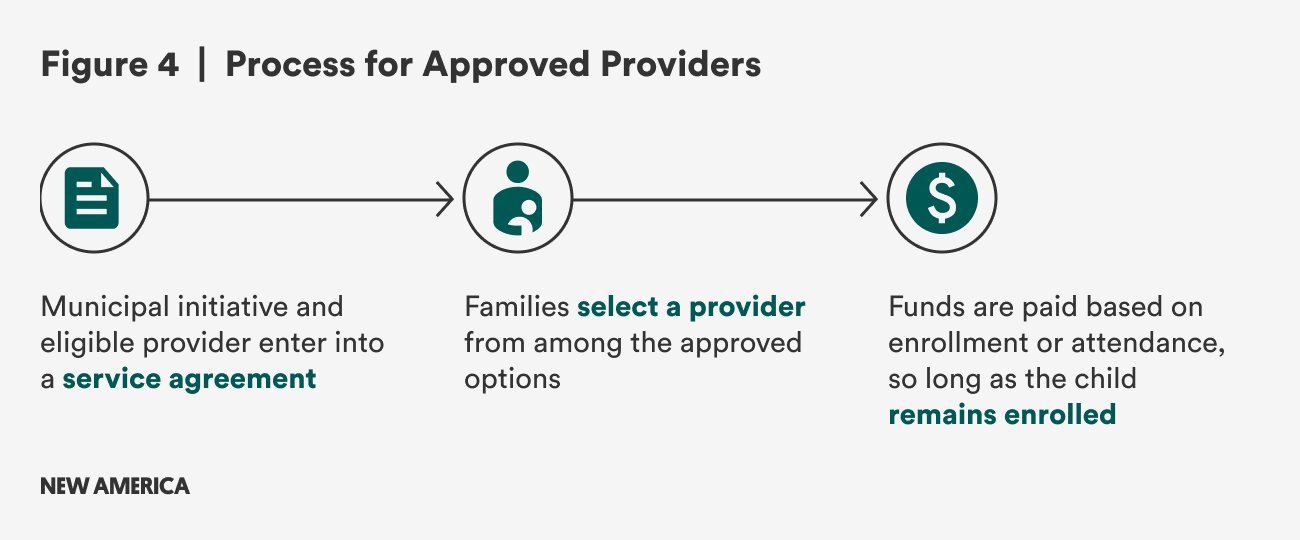
When private child care providers opt into a publicly funded system, it can mean different things depending on the geography. In some places with contracted models—like Philadelphia, Seattle, and Multnomah County—the city or county administrator enters into a contract with the provider, reserving a certain number of seats for children and either guaranteeing funding for those seats or promising to fund them if the seats are filled (see Figure 3 below). In other places with approved provider models—like Cincinnati, San Francisco, and Denver—there are no seat guarantees, and providers only receive funding for as long as an eligible child attends the program (see Figure 4 below). In both contracted and approved provider models, there are different ways to approach payment; providers can be paid based on attendance, enrollment, or a set grant or contracted amount.
Contracted Models
Contracted models typically offer providers greater predictability and stability, and may give program administrators a greater degree of control over what happens in classrooms. However, providers may struggle with a loss of autonomy. Families may feel like their choices are more constrained if they want to access a publicly funded program and their provider of choice is not one of the options. When participating providers have a minimum number of seats they must offer to have a contract, for example, it means a smaller total number of participating providers.
For the administering agency, the administrative costs and complexities to managing a contracted program can be higher than a voucher program. On the other hand, it can streamline some processes because there is more consistency in provider participation and a greater ability to mandate specific policies and procedures.
Approved Providers
In programs where families select their provider and funding follows them, families may have the ability to choose among a greater number of providers. Providers may have a looser relationship to the overall program and retain more control over day-to-day operations. Some providers prefer to serve a mix of publicly funded children and private-pay children because they are not reliant on a single revenue source. However, in such a fragmented system, it may be more challenging to maintain consistency in approach across providers, particularly if some providers have just a few children from the locally funded program in each classroom. Providers may also struggle to meet the programmatic requirements of the initiative if they are only funded for a child or two, but expected to meet classroom-wide requirements like minimum teacher credentials.
Some places seek a middle ground between these pathways by requiring participating providers to allocate a certain number of slots to the publicly funded program, even if it does not amount to a fully dedicated classroom.
Approaches to Provider Payment
Within contracted programs, providers are typically paid based on attendance, enrollment, or the number of slots in their contract, regardless of whether they are filled. Attendance-based payment is the most fiscally conservative approach, but has become far less typical, particularly following the COVID-19 pandemic. Enrollment-based funding is the most common approach across state preschool programs and local early childhood initiatives. This aligns to how public school funding works in most states, to new guidance for federal child care subsidy funds (at least as of publication of this report), and to how most private child care fees are managed. Some system leaders have found that enrollment-based payment may create more incentive for providers to work to fill slots. Payment may be tied to enrollment at a single point in time during the school year or assessed on a more frequent basis.
However, many providers would argue that enrollment-based payment does not fully align with their operating model, as the high fixed costs in early education (staffing and rent) go unchanged whether there are 12, 15, or 18 children in the classroom. Some systems have recognized this and shifted to pay providers based on the seats in their contract without pegging payment to enrollment. For some, this may raise questions about fiscal waste—why should the city or county pay for unused slots? However, system leaders have other levers to encourage providers to increase enrollment and to reduce overpayment, such as reducing the number of slots in a provider’s contract if underenrollment is persistent.
How Are Provider Payment Rates Set?
The other aspect of provider payment is how per-child rates are set, and to what extent that varies within a mixed delivery model.
Per-child rates may vary based on multiple dimensions, including:
- Program schedule: Within a single system, some providers may operate on a school day and year calendar, whereas others may operate for the full working day and calendar year.
- Provider type: The fixed costs to provide care are often higher in center-based programs than home-based settings. Most state child care subsidy programs pay a higher per-child rate to centers than homes, which influences local rate setting.
- Provider quality rating: Running a high-quality program may cost more in staff salaries, materials, and other expenses. Some believe that paying a differential rate based on quality will incentivize providers to pursue higher quality ratings, and this differentiation is built into many state child care subsidy payment models as well.
- Age of child: Due to smaller class sizes, it is more expensive to operate a classroom for toddlers than preschoolers, for example.
- Fixed provider costs (e.g., rent): Within a locality, there may be significant enough differences in facilities cost that there is a need to address it within the funding formula. Similarly, there may be meaningful differences in staff costs across providers, particularly if programs are bound to union-negotiated collective bargaining agreements that differ by staff title and credential.
- Population risk factors (e.g., homelessness): Programs may incur additional cost to provide more comprehensive services to address the challenges that children and families are facing.
- Specific student needs (e.g., students with disabilities, dual language programs): Specific services may carry additional costs based on different staffing, supply, material, and technology needs.
Systems that have greater variation in their rates recognize the differential costs to running different program models, but they risk creating additional administrative complexity for their central office staff. Systems with greater uniformity in their rate structure are able to communicate more simply with providers and run a more streamlined operation, but there is risk that some providers will not receive sufficient funds to operate their program.
In New York City, the per-child rate paid to private providers is highly customized; per-child rates are individually negotiated with each center-based provider to allow for variation in costs. This gives the system flexibility, particularly around rent and staffing costs, which vary widely across the city. Home-based provider rates are fixed and tied to the state’s child care market rate formula. School district classrooms are funded through a different mechanism. There is no differentiation based on quality in any setting.
In Multnomah County, all providers receive the same rate for three- and four-year-olds, regardless of setting or other characteristics; the only variation is for providers who operate for a school day and year versus those who operate for the full working day and full calendar year. This approach has been lauded by home-based providers in particular, who are often paid a much lower rate than center-based providers in other systems.
An argument could be made that both approaches can drive toward equity—and also that in either model, some providers may be left behind. In a model that is highly differentiated, providers with greater business savvy may be able to better advocate for themselves during the budget negotiation process. In a model that is highly uniform, providers with higher-than-average fixed costs may struggle to make the numbers work. One model may be a better fit over another for a particular locality based on the level of variation in fixed costs, the range of different program models that are offered, and the precedent set by other state and local funding streams. In any approach, system leaders can work toward equity by using real data on the actual cost of care and providing sufficient funds for all providers to meet expectations and create a high-quality learning environment.
Beyond meeting the bare minimum, system leaders could also consider how rate structures and differentiation in rates can incentivize special programs that meet specific needs. For example, providers who implement robust two-generation programming that includes services for caregivers could receive a rate bump. Standardization leaves little room for experimentation and innovation; there is value to encouraging and replicating bright spots.
What Role Does the School District Play?
School districts play a very different role than private providers. In many localities, they are essentially guaranteed the right to provide preschool services; by contrast, private providers often have to compete for that opportunity. They are not coming into mixed delivery models fearful for their own survival and livelihood; this power imbalance sets the tone for many of the tensions that system leaders face in navigating the role that school districts play.
Structurally, districts play a few different roles across locally funded mixed delivery early childhood programs:
- Administrator and service provider: The district manages state and local early childhood funds, operates services, and contracts with private providers to offer some services.
- Service provider: Another entity (city or county agency, independent agency) administers early childhood funds; the district is one of multiple providers.
- Service provider, with role in governance: The district is one of multiple providers and has some role in governance (e.g., designated positions on program board).
- Opts out: The district provides early childhood services that are distinct and separate from the city or county early childhood initiative (or provides no services at all).
Of course, the distinctions are not so clean. In many communities in the ECE Implementation Working Group, there are multiple school districts, or the school district or districts engage in multiple ways, across different funding streams. In San Antonio, the local preschool program, Pre-K 4 SA, partners with seven of the 17 independent school districts that serve parts of the city.
Regardless of the specific structural role, districts can play many different functional roles to support local early childhood services across settings. In many ways, the scale, expertise, and resources of the school district can benefit the full system. Some of these functional supports can include quality assurance and support, including professional development, evaluation, and coaching; coordination and system building, including management of centralized enrollment systems and curricular alignment across pre-K and K–12; family engagement and outreach; and policy and advocacy. School districts can also create capacity for early childhood providers to run their programs in vacant classrooms in school buildings or identify creative solutions for co-location, particularly as school enrollment declines in many communities.
What Are the Expectations of Providers and Supports Available to Meet Them?
For leaders of mixed delivery models, there are many detailed design decisions that go into building a system that drives equity and quality for all participants. Different systems vary in how much they prescribe what happens in private programs that take public funding. Some of these design questions include:
- What are the administrative and operational policies that all providers will be required to meet? How, if at all, will that vary by setting? Examples of such policies would be specific protocols around daily schedule, programmatic calendar, teacher hiring and staff management, and use of specific child data systems. Some localities allow providers a fair amount of discretion in these decisions; others define detailed policy requirements and hold providers accountable to meet them. How family enrollment happens and what controls are given to individual providers versus the central administration is a critical design decision. (See our prior brief on building centralized enrollment systems in local early childhood programs.)
- What instructional requirements do providers need to meet? Are specific curricula required? Many places define learning standards or lean on state-defined standards. Some localities specify a single curriculum or define a menu of allowable choices; others leave the choice open-ended. Providers may be able to opt into specific instructional models, such as dual language instruction, and more detailed guidance may be given for what inclusive settings for children with disabilities should look like.
- How should providers assess student progress? Some localities mandate the use of particular learning assessments for students, both to inform instruction and to measure impact at the end of the program year (e.g., Kindergarten Readiness Assessments). Localities vary in whether they collect and analyze data from these assessments centrally.
- How will provider quality be monitored and measured? If mixed delivery early learning requires quality rating participation for providers, leaders will need to plan for scaling up existing systems and potentially tailoring them for different care settings. Some localities define their own measures of quality. Program administrators will also need to determine how this information is used, including whether it is made available transparently to families.
- What support will be available to providers? Some localities offer robust professional development to educators and leaders, including on-site coaching, and operational support to child care business owners. Others primarily rely on state-funded or -provided professional development.
- What happens if a provider does not comply with policy or instructional requirements? Localities will need defined protocols and processes to address issues that may come up with providers, including what happens to their ability to remain a contracted or affiliated provider if there is a license suspension, a concern about instructional quality, or a breach of contract.
In a prior brief, we explored the benefits of participatory planning in systems design. Inviting providers into the process to answer these questions and shape the local approach can increase buy-in and lead to a stronger program model.